


Sheila Hustadi Budiawan1; Abraham Arimuko2; Lilik Norawati2; Asnawi Madjid1; Widya Widita1
Financial support: None.
Conflict of interest: None.
Submitted on: 20/10/2022.
Approved on: 20/09/2023.
How to cite this article: Budiawan SH, Arimuko A, Norawati L, Madjid A, Widita W. Treatment of periorbital syringoma with intradermal botulinum toxin A monotherapy versus carbon dioxide laser: a case report. Surg Cosmet Dermatol. 2024;16:e20240190.
Syringomas are benign adnexal neoplasms that develop from eccrine sweat ducts. They are mostly found in early adulthood, with a female gender predominance. They typically occur on the face, particularly the periorbital region, which has a high demand for cosmetic enhancement. Management of periorbital syringomas is challenging, with no consistently effective treatment available. Intradermal injection of botulinum toxin A (BTX-A) is a new treatment modality for periorbital syringoma. We present a 53-year-old female patient with periorbital syringoma who was successfully treated with intradermal BTX-A monotherapy as a painless, cost-effective treatment that produced better long-term results than carbon dioxide laser.
Keywords: Botulinum Toxins, Type A; Syringoma; Carbon Dioxide
Syringomas are benign adnexal neoplasms that arise from eccrine sweat duct. The lesions manifest as small, hard, flesh-colored or yellow papules, often in multiples, with a symmetric distribution.1 They are most common in early adulthood, with a female predominance, and are commonly found on the face, particularly the lower eyelids. Lesions in sensitive areas such as the periorbital region can cause psychological distress, so cosmetic repair is in high demand.2,3
Multiple therapeutic approaches have been attempted, including surgical procedures such as dermabrasion, excision, cryotherapy, electrocautery, electrofulguration, laser therapy, and chemical cautery, with the carbon dioxide (CO2) laser being the most commonly used ablative laser therapy. All these approaches carry a significant risk of recurrence.2,4
Nonsurgical alternatives such as topical retinoids, dermabrasion, and intradermal botulinum toxin A (BTX-A) monotherapy have been used in the management of periorbital syringoma, but only in isolated case reports or small case series.5,6 This entity continues to pose a therapeutic challenge, with no consistently effective treatment available.7
We present a case of a 53-year-old female patient with periorbital syringoma who was successfully treated with monotherapy intradermal BTX-A and showed superior result compared to CO2 laser.
A 53-year-old female visited the Dermatology and Venereology clinic with a 9-year history of 1-to-3-mm, skin-colored papules in the area around the eyes. Initially small, the papules grew larger gradually. Despite no pain or pruritus, the lesions bothered her cosmetically. The patient had undergone CO2 laser treatment 5 years before, but the lesions recurred. On dermatological examination, numerous skin-colored papules consistent with syringoma were seen in the periorbital region.
The patient consented to a split-face procedure using CO2 laser on the left periorbital area and intradermal BTX-A on the right periorbital area. Written consent was obtained. Ablative CO2 laser was performed on the left periorbital area until the syringoma resolved, with topical anesthesia given 30 minutes prior to the procedure. A 100-unit vial of BTX-A was diluted in 2.5 mL of preservative-free normal saline solution. A total of 24 international units (IU) were intradermally distributed using a 30 G×4mm needle and 1-cc syringe into 1-cm2 injection sites in the right periorbital area (2 IU per site), with ice application prior to injection. In comparison to CO2 laser therapy, the patient found intradermal BTX-A injections to be more comfortable and less painful.
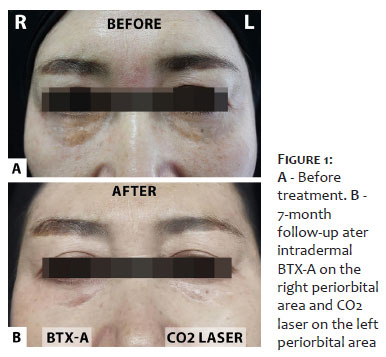
Significant improvement of the syringoma was achieved by both treatment modalities within different time frames. On the left periorbital region, which was treated by CO2 laser, the lesion disappeared immediately, with a wound healing time of about 2 weeks, and reappeared 4 months later. On the right periorbital area, which was treated using intradermal BTX-A, improvement progressed gradually, with no reappearance at 7-month follow-up. (Figure 1)
Syringomas are benign adnexal tumors that clinically appear as yellowish or skin- colored papules 1-3 mm in size, most typically found in the lower periorbital region, and can cause significant cosmetic concerns. The goal of treatment is to improve appearance by eradicating the tumor in a minimally invasive fashion. Numerous treatment strategies with varying degrees of success have been described in the literature; the most common problem in the management of syringoma is recurrence.7
Botulinum toxin A is a neurotoxin with numerous dermatological applications which inhibits acetylcholine release from cholinergic nerve endings. This leads to chemodenervation, which modulates the autonomic regulation of eccrine glands.8 BTX-A is being studied as a novel treatment modality for various skin conditions, including hyperhidrosis, hypertrophic scars and keloids, Raynaud phenomenon, oily skin, facial flushing, psoriasis, and cutaneous lesions (including periorbital syringomas).9
Although the exact mechanism by which BTX-A affects syringoma is unknown, it could be explained by inhibition of the SNAP-25 (synaptosomal associated protein of 25 kD) component of the SNARE (soluble N-ethylmaleimide-sensitive factor attachment protein receptor) complex, which prevents the release of acetylcholine from vesicles within the cytoplasm of nerve endings. This causes suppression of cholinergic terminals on autonomic nerves, which in turn control the secretion of eccrine sweat glands, from which syringoma is derived.6 CO2 laser, on the other hand, destroys the syringoma itself as the target tissue by heating and vaporizing intracellular water, but is associated with a high potential of recurrence. When employed fractionally, CO2 laser remains the treatment of choice, with intralesional electrocoagulation available as a second option with acceptable results and lower risk of complications.7 A review article reported that CO2 laser is the most commonly used ablative laser therapy; however, it is frequently associated with side effects such as scarring and dyspigmentation.2,5 Previous clinical research with CO2 laser showed that the fractional ablative method resulted in post-treatment erythema lasting a mean of 16.67 days, crusting for a mean of 5.87 days, and post-treatment hyperpigmentation in 14.3% of patients.10
In a retrospective study of 92 patients, Seo et al. compared CO2 laser therapy with multiple perforations combined with botulinum toxin A. In a previous study, the authors had reported success with deep tumor eradication using a CO2 laser with multiple perforations ("multiple-drilling method"), and in this later series, decided to add botulinum toxin A as an adjunct. Although the rate of recurrence was comparable in both groups, the rate of improvement was much higher in the combination therapy group.8
Fujigaki reported a case of localized syringomas in the periocular and upper lip region treated with 46 IU of BTX-A intradermally as monotherapy. At 8-month follow-up, the patient showed significant improvement.6
Intradermal BTX-A monotherapy could potentially become the treatment of choice in the management of syringoma, allowing selective eradication of dermal target lesions while preserving normal epidermal tissue.3 In this case report, it was also shown to be a painless treatment with a better long-term outcome than carbon dioxide laser.
Intradermal BTX-A injection offers a painless and more cost-effective treatment option with better long-term outcomes compared to carbon dioxide laser in the management of periorbital syringoma.
Sheila Hustadi Budiawan
ORCID: 0000-0001-6407-8489
Approval of the final version of the manuscript; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in reasearch guidance; critical review of the literature; critical review of the manuscript
Abraham Arimuko
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases
Lilik Norawati
Approval of the final version of the manuscript; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript
Asnawi Madjid
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript
Widya Widita
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript
1. Foreman RK DL. Appendage tumors of the skin. In: Kang SAM, Bruckner AL, Enk AH, Margolis DJ, McMichael AJ, Orringer JS. Fitzpatrick's dermatology. 2nd ed. New York (USA): McGrawHill; 2019.
2. Alsaidan MS. Efficacy and safety of lasers in treating syringomas: a review of the literature. J Dermatolog Treat. 2022;33(8):3127-35.
3. Ahn GR, Jeong GJ, Kim JM, Hong JY, Li K, Lee CK, et al. Intralesional electrocoagulation with insulated microneedle for the treatment of periorbital syringomas: a retrospective analysis. Aesthet Surg J. 2021;41(4):490-8.
4. Sharma A, Subburaja K, Kumaran MS. Pigmented papules on the face, neck, and chest. 2022;110(2):63.
5. Srimuang A, Sooksamran A, Boonpuen N. A possible new variants of familial Syringoma: case reports and review of literature. Thai J Dermatol. 2022;38(2):65-74.
6. Zaldivar‐Fujigaki JL, Achell Nava L. Botulinum toxin A as monotherapy for syringoma. J Cosmet Dermatol. 2021;20(5):1393-5.
7. Claro KTV, Ramirez JLH, Haddad A, Cunha MGD, Francischeli Neto M. Treatment of periorbital syringomas: review of the scientific literature in the last 5 years. Rev Bras Cir Plást. 2022;37(1):80-8.
8. Seo H-M, Choi J-Y, Min J, Kim W-S. Carbon dioxide laser combined with botulinum toxin A for patients with periorbital syringomas. J Cosmet Laser Ther. 2016;18(3):149-53.
9. Guida S, Farnetani F, Nisticò SP, Mariarosaria CG, Babino G, Pellacani G, et al. New trends in botulinum toxin use in dermatology. Dermatol Pract Concept. 2018;8(4):277.
10. Lee SJ, Goo B, Choi MJ, Oh SH, Chung WS, Cho SB. Treatment of periorbital syringoma by the pinhole method using a carbon dioxide laser in 29 Asian patients. J Cosmet Laser Ther. 2015;17(5):273-6.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}