


Naomi Carrara Matsuura; Cibele Toledo; Victoria Linhares Maia Santana; Denise Steiner; Nabila Scabine Pessotti
Submitted on: 23/08/2023
Approved on: 07/01/2024
Financial support: None.
Conflict of interest: None.
How to cite this article: Matsuura NC, Toledo C, Santana VLM, Steiner D, Pessotti NS. Intense pulsed light therapy for treatment of facial erythema and hypertrophic scar after phenol peeling. Surg Cosmet Dermatol. 2024;16:e20240292.
Facial erythema after phenol peeling is one of the expected effects of the healing process and collagen formation. Intense Pulsed Light (IPL) therapy is one of the forms used as a treatment accelerating recovery, reducing redness, inflammation, and itching symptoms that may occur after peeling. IPLT can also be used to treat hypertrophic scars, which is also one of the adverse events that can happen with deep peeling. We report a successful case of IPLT treatment in a patient who presented facial erythema and hypertrophic scarring after undergoing phenol peeling.
Keywords: Phenol; IPL treatment; Hypertrophic Scar.
Facial erythema is one of the most common outpatient complaints in Dermatology. There are several causes of facial erythema, which can be physiological and transient or occur in diseases such as rosacea, lupus erythematosus, and dermatomyositis.1 Facial erythema can also occur as an adverse event after phenol peeling, currently used to treat deep wrinkles and severe acne scars. Phenol is a deep peeling that immediately coagulates superficial epidermal and dermal proteins with a histological increase in collagen and elastic fibers.2
Prolonged post-phenol peel erythema is benign. It begins during the first week and peaks in the second week after the procedure. Erythema is a normal part of the healing process and is a sign of reticular dermal collagen formation. Patients typically present this condition within three to six months and up to a year during exercise.3 The formation of hypertrophic scars can occur in specific areas, such as the zygomatic arch, pre-auricular region, medial upper eyelids, lower eyelids, and neck, where the peeling should be less vigorous.3
Intense Pulsed Light (IPL) therapy is a light device commonly used to treat these conditions of facial erythema and hypertrophic scars.1,4 This light emits wavelengths between 420 nm to 1400 nm. It emits the wavelength needed to target specific chromophores and improve penetration by using filters, thus minimizing energy absorption by other chromophores. Advantages of the IPL system include lower cost, versatility to target multiple chromophores, flexible parameters with less complexity, and fewer adverse events.5 Incorrect patient selection, i.e., skin color or ethnicity, is a significant cause of burn injury as there are variations in melanin content in different people.1
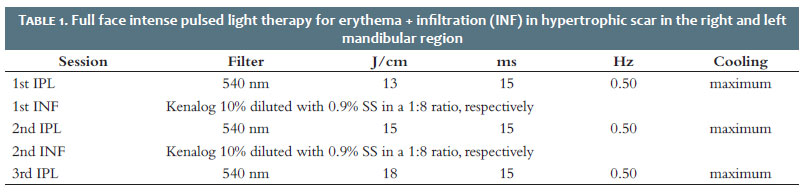
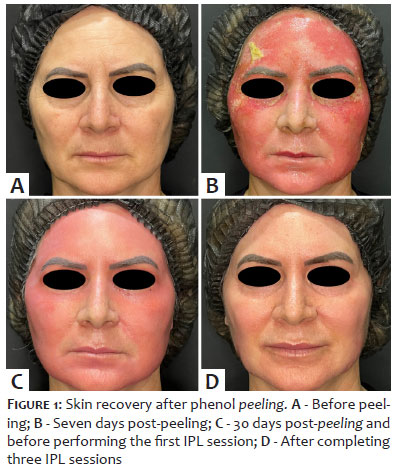
A 52-year-old woman, Fitzpatrick skin phototype II, presented facial erythema and hypertrophic scar after undergoing phenol peeling with Hett formula 1.2% to treat photoaging and periocular wrinkles. Three IPL sessions were performed on the entire face at monthly intervals, one month after the deep peeling, using parameters as shown in table 1 and photographic monitoring before and after each procedure (Figure 1).
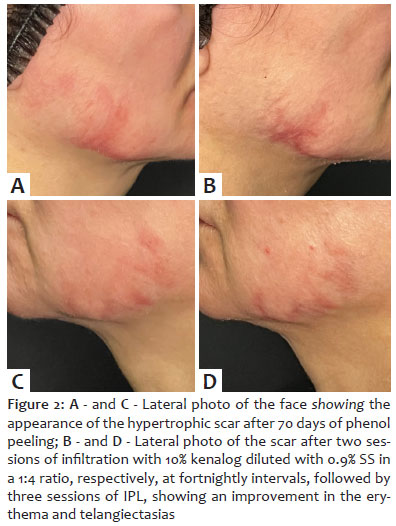
During the laser sessions, the patient developed a hypertrophic scar in the mandibular region bilaterally, one of the most feared complications of phenol peeling. Between IPL sessions we conducted two infiltrations using 10% kenalog diluted with 0.9% saline solution (SS) in a 1:8 ratio, respectively, with fortnightly intervals, always one week before the IPL sessions, resulting in improvement of erythema and telangiectasias (Figure 2).
After the three IPL sessions, we observed a reduction in facial erythema and an improvement in the appearance and symptoms of itching in the hypertrophic scar in the mandibular region on both sides of the face through the photographic comparison. Although the patient had post-peeling adverse events, she obtained the desired improvement in her deep periorbital wrinkles, reporting that she was satisfied with the result after all the procedures (Figure 3 to 6).
Phenol has been used as a deep peeling both alone and in association with other components that act as penetration and permeation promoters. These products result in an intense cell renewal process, normalizing skin pigmentation, reducing marks, and minimizing wrinkles.6 Prolonged erythema may persist for a period ranging from three to six months after the deep peeling.3 Furthermore, IPL can treat telangiectasias resulting from the dilation of capillary microvessels. In this case, its mechanism of action is based on photothermolysis, or thermal damage to the vessels, which induces intravascular coagulation.7
Scars can occur after peeling and can be permanent. They generally appear in regions such as lips, eyelids, and jaw.6 The mechanism of action of IPL in hypertrophic scars is not fully understood, but it probably targets vascular proliferation essential for excessive collagen production. Wavelengths from 400 nm to 600 nm impact the vasculature directly, reducing its thickness and inhibiting its growth. It also heats the dermal collagen fibers, promoting their contraction and improving the texture of scars.7
In 2014, Meymand assessed the use of IPL associated with intralesional corticosteroids in the treatment of 86 patients with hypertrophic scars and keloids. The study held eight sessions every three weeks. According to the paper, the association between treatments accelerated results without presenting significant adverse events, with a degree of clinical improvement considered excellent in 73% of cases.7
Complications from phenol peeling are a challenge for dermatologists, and it is necessary not only to identify them early but also to know how and when to intervene. Intense pulsed light (IPL) therapy is a proven effective technique to treat facial erythema and hypertrophic scars. Therefore, it is critical to deepening the knowledge of IPL to optimize the application techniques, keeping in mind that combining techniques results in greater comfort and requires a smaller number of sessions.7
Naomi Carrara Matsuura
ORCID: 0000-0001-5097-6851
Statistical analysis; approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Cibele Toledo 0009-0005-1014-7705
Preparation and writing of the manuscript; collecting, analyzing, and interpreting data.
Victoria Linhares Maia Santana 0009-0000-6597-1463
Collecting, analyzing, and interpreting data.
Denise Steiner
ORCID: 0000-0001-6450-9234
Critical review of the manuscript.
Nabila Scabine Pessotti
ORCID: 0000-0003-0879-2981
Effective participation in research guidance; critical review of the manuscript.
1. Yepuri V, Patil AD, Fritz K, Salavastru C, Kroumpouzos, Nisticò SP, et al. Light-based devices for the treatment of facial erythema and telangiectasia. Dermatol Ther (Heidelb). 2021;11(6):1879–1887.
2. Lee KC, Wambier CG, Soon SL. Basic chemical peeling: superficial and medium-deph peels. J Am Acad Dermatol. 2019;81(2):313-324.
3. Wambier CG, Lee KC, Soon SL, Sterling JB, Rullan PP, Landau, et al. Advanced chemical peels: Phenol-croton oil peel. J Am Acad Dermatol. 2019;81(2):327-336.
4. Abalí MO, Bravo BSF, Zylbersztejn D. Intense Pulsed Light in the treatment of scars caused by burns. Surg Cosmet Dermatol. 2014;6(1):26-31.
5. Handler MZ, Bloom BS, Goldberg DJ. IPL vs PDL in treatment of facial erythema: a split- face study. J Cosmet Dermatol. 2017;16(4):450-453.
6. Velasco MVR, Okubo FR, Ribeiro MR, Steiner D, Bedin V. Rejuvenescimento da pele por peeling químico: enfoque no peeling de fenol. An bras Dermatol. 2004;79(1):91-99.
7. Kalil CLPV, Reinehr CPH, Milman LM. Luz Intensa Pulsada: revisão das indicações clínicas. Surg Cosmet Dermatol 2017;9(1):9-17.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}