


Thalita Machado Carlesso1; Lorena Visentainer2; Bárbara Elias do Carmo Barbosa3; Thais Oliveira Reis1; Camila Cavalcanti Freitas2
Submitted on: 27/03/2023
Approved on: 19/10/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Carlesso TM, Visentainer L, Barbosa BEC, Reis TO, Freitas CC. Eyebrow transplant using the Follicular Unit Extraction Technique (FUE). Surg Cosmet Dermatol. 024;16:e20240239.
Hair transplant is a common procedure worldwide, and the method of extracting follicular units is currently the most used. This technique is used not only for androgenetic alopecia but also for other areas such as eyebrows and beard. It is essential to observe the angle of the incisions and implantation of the hairs to conduct the eyebrow transplant so the result is as natural as possible. However, in addition to being rigorous with the design of the shape and position of the eyebrow, care must be taken with the preparation from the receiving site.
Keywords: Transplants; Alopecia; Hair follicle
The trend for thicker eyebrows, with greater visual and aesthetic appeal, has increased patient demand for eyebrow transplants in recent years. Hair restoration in this region represents a very refined art, requiring a high skill to be correctly executed, as it is necessary to respect the arrangement and positioning of the hair to obtain a good result.1
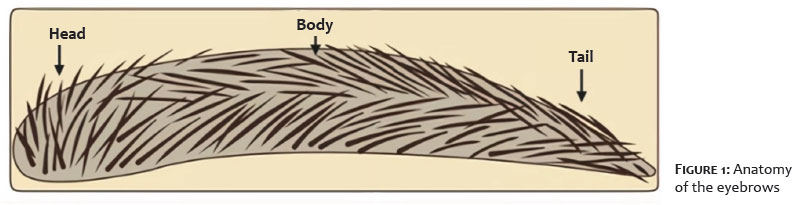
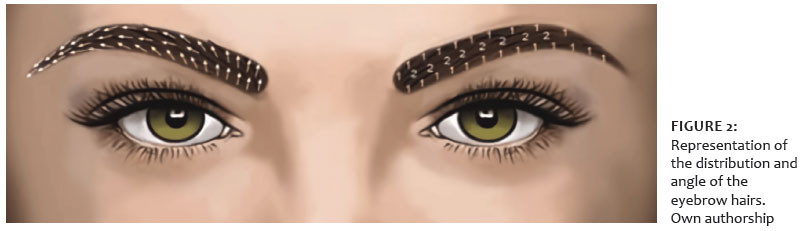
The eyebrows have biological functions, such as protecting the eyes and helping with facial expressions.2 They can be divided into three anatomical segments: head, body, and tail. Its hairs are generally shorter, thinner, and less flexible, with a slight curvature along the body. Furthermore, its shape tends to be slightly thinner towards the tail. Regarding the orientation and density of the hair, each segment has its own particularities.3 (Figures 1 and 2)
The most common indications for eyebrow transplant are burns, trauma, alopecia areata, scarring alopecia (such as frontal fibrosing), trichotillomania, hypothyroidism, leprosy, and hypotrichia.5,6,7 However, it is essential to highlight that, in some of these conditions, such as alopecia areata, frontal fibrosing alopecia, and trichotillomania, careful medical evaluation is necessary to ensure there are no signs of disease activity for proper scheduling of the surgical procedure.1,8
Eyebrow transplant surgery is performed using the follicular unit extraction (FUE) technique, currently considered the best option for restoring this region.9
The procedure begins with a small scrape of the donor region (generally the occipital region of the scalp), followed by asepsis with chlorhexidine degerming agent in sufficient quantity to clean the area. Then, the anesthetic solution is infiltrated, which, considering an average of 70 kg of patient weight, is prepared with 10 ml of 2% lidocaine without vasoconstrictor, 20 ml of 0.75% ropivacaine and 0.3 ml of adrenaline (300 mcg). Thus, this total volume of anesthetic will be used both in the donor region (scalp) and the recipient region (eyebrows) later. The amount of anesthetic will depend on the size of each area, and the doctor must be careful to inject only what is necessary, avoiding large doses of the medication. Also, a small amount of tumescent solution can be applied, consisting of a mixture of 100 ml of Ringer's lactate solution and 0.3 ml of adrenaline to help the vasoconstriction of the area and superficialize the follicles to protect the deeper blood vessels during extraction. In general, 4 ml of this solution is already satisfactory for use in the donor region.
Follicular extraction uses the FUE technique, preferably with a 0.9 mm punch. The number of follicular units to be extracted depends on the size of the recipient region that will be covered in the transplant. Each eyebrow may require, on average, 150 to 300 follicles for a complete and well-done reconstruction. Furthermore, the preference is to use follicular units with one and two hairs, while those with three and four hairs must be cut and transformed into smaller units.
After extraction, the patient remains in the prone position for better access to the eyebrow region. Then, we conduct the asepsis and local anesthetic infiltration in the recipient region using the same previously prepared solution; however, in a smaller quantity and proportional to the area where it will be implanted. It is a highly innervated site (due to the presence of the infratrochlear, supratrochlear, supraorbital, lacrimal, and zygomaticotemporal nerves) and, therefore, this stage is essential for the patient's comfort throughout the surgery. A small volume of corticosteroids, such as triamcinolone acetonide, can be added to the anesthetic solution to reduce the periorbital edema that may occur in some cases. However, this practice is not essential and depends on the surgeon's preference.
The next step consists of pre-incisions (Figure 3) using 0.8 mm sapphire scalpel blades, 0.7 mm customized blades, or 23 G needles at a 90-degree angle (Figure 4). The detail of this step is that the cuts must occur at a very acute angle concerning the skin, following the direction of the existing hair in each region.
The incisions are made in the coronal axis to facilitate the implantation of the follicles, but the direction may vary depending on the anatomy of each part of the eyebrow. At the medial end, a few staggered rows are created so the hair grafts are placed pointing upwards. As they reach the body, the slits slope outward and downward along the upper edge of the eyebrow while becoming parallel to the middle rows. Then, they slope downward toward the tail.
Two lines placed in this pattern along the top edge will define and highlight the curvature of the eyebrow. Then, other two lines are placed horizontally along the longitudinal axis for proper body structure. Finally, two more lines of slits are created along the bottom edge so the grafts can be at right angles to the top edge, creating a crisscross pattern that overlaps along the central axis.
Because women's eyebrows are thinner and more curved, the total number of rows in women is generally smaller. But, in any case, it depends on the patient's desire for the final result. Thinner follicles are preferred for the upper edge and tail, while thicker ones are placed along the body and lower edge.
It is essential to implant the grafts close to the skin so the growth of the hairs does not affect the region's harmony. After applying a small amount of methylene blue to the pre-incisions, they become more visible, making the implantation process easier. Generally, 0.65 mm implants are used for single-hair units and 0.8 mm for two-hair follicular units.
In the post-operative phase, it is recommended to hydrate the region with the application of thermal water every hour after the procedure for at least one day. Cleaning must take place delicately after 24 hours with a drain rinse, and it is not necessary to apply bandages throughout the recovery process. Regarding oral medications, the recommendation is prophylactic antibiotics for seven days (such as cefadroxil, with a dose of 500mg every 12/12 hours) and dexamethasone 4 mg per day, for five days, to reduce local edema.
Transplanted follicles grow at different speeds as they are in different hair cycle phases. A partial result (on average 50%) is expected three to four months after the procedure. Eight to nine months is necessary to obtain the result, with complete restoration of the eyebrows.
Depending on the needs of each case, a second session can be planned after an average of ten months. However, many patients already meet their expectations in the first surgery when the technique is performed correctly and the postoperative period is uneventful.
Figures 5, 6, and 7 show eyebrow transplant results on different postoperative days.
Hair transplant is a procedure highly sought in Dermatology and Trichology. Patients are seeking the surgical procedure following the trend towards thicker, more natural-looking eyebrows. Previously used techniques, such as eyebrow micropigmentation, are becoming less and less attractive since their results are more artificial and do not value the individuality of each patient, which further favors the search for other alternatives, such as transplants.
The FUE technique allows a more natural restoration than other surgical techniques, guarantees a more thorough follicular extraction, and is minimally invasive. Furthermore, it favors a smoother recovery for patients, with excellent results.
The strategic distribution of follicular units is directly related to the density of the eyebrows, and it is crucial for patient satisfaction. For the implantation of the hair, it is essential to maintain a more acute angle concerning the skin, following the direction of pre-existing threads when these are present.1,8
When the eyebrows already have some previous scar tissue, whether due to old trauma or specific types of alopecia, performing a hair transplant is a challenge for the surgeon due to the compromised vascularization in this region. Therefore, it is more difficult to predict the degree of success regarding follicular integration in these patients.10
All types of measures must be considered to improve graft viability during the surgical procedure. Bleeding at the incision site can lead to displacement of the follicles and changes in angle and direction, which can impact the final result. This event is common when there are (recent) pink scars in the eyebrow area. Therefore, even if patients insist on undergoing the transplant early to correct this change, doctors must wait for the scars to mature. Additionally, some fat grafting may be applied before surgery to soften the hard layer of scar tissue or in patients with insufficient skin area.10
Successful results are achieved when all factors with potentially adverse events on graft viability are considered. Thoroughly planning the surgery and avoiding additional intraoperative trauma also contribute to the success of the procedure.10
Some patient particularities can influence the shape of the eyebrows, such as the variability between ethnicities and gender.4 For example, in women they are a little thinner than in men, in addition to presenting in a "C" shape, reaching maximum curvature at the most lateral edge.9 Men's eyebrows tend to be less arched, with the medial and lateral ends practically level or even with the tail slightly higher.9
A few months after surgery, there may be a need to trim the new hairs more frequently. After all, the anagen phase of the scalp follicles (donor area) is greater, and the transplanted hairs follow their original pattern, even though they are in a new region.
Eyebrows play an important role in harmonizing the face and, currently, they tend to be increasingly fuller and more shaped, which justifies the greater interest of patients in hair transplants in this region.
The FUE technique is currently the most appropriate methodology for reconstructing this region, being the primary choice of doctors, both for reducing surgical trauma to the follicular units and for delivering more natural results.
Eyebrow transplants are becoming more widespread in medical practice and gaining prominence among patients seeking more effective procedures. Furthermore, restoring the eyebrows permanently is an advantage of the technique. Thus, a well-trained doctor will be in the spotlight in hair and eyebrow restoration.
Thalita Machado Carlesso
ORCID: 0000-0003-2078-305X
Preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Lorena Visentainer
ORCID: 0000-0003-2706-3098
Approval of the final version of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
Bárbara Elias do Carmo Barbosa
ORCID: 0000-0001-8559-0852
Critical literature review; critical review of the manuscript.
Thais Oliveira Reis
ORCID: 0009-0002-2216-6020
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Camila Cavalcanti Freitas
ORCID: 0000-0002-0787-6828
Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
1. Lam SM. Hair loss and hair restoration in women. Facial Plast Surg Clin North Am. 2020;28(2):205-23.
2. Bared A. What's new in facial hair transplantation?: effective techniques for beard and eyebrow transplantation. Facial Plast Surg Clin North Am. 2019;27(3):379-84.
3. Epstein J, Bared A, Kuka G. Ethnic considerations in hair restoration surgery. Facial Plast Surg Clin North Am. 2014;22(3):427-37.
4. Tom CM, Malouf PJ. Eyebrow restoration: the approach, considerations, and technique in follicular unit transplantation. J Cosmet Dermatol. 2015;14(4):310-14.
5. Epstein J. Facial hair restoration: hair transplantation to eyebrows, beard, sideburns, and eyelashes. Facial Plast Surg Clin North Am. 2013;21(3):457-67.
6. Figueira E, Wasserbauer S, Wu A, Huilgol SC, Marzola M, Selva D. Eyebrow reconstruction. Orbit. 2017;36(5):273-84.
7. Gandelman M. A technique for reconstruction of eyebrows and eyelashes. Semin Plast Surg. 2005;19:153-8.
8. Noori A, Rabiee M, Mehrabani D, Namazi MR. Head and neck restoration in scar Alopecia: hair transplantation in scalp, eyebrows, beard and mustache. World J Plast Surg. 2021;10(3):90-8.
9. Rajput RJ. Hair transplant for eyebrow restoration. Indian J Plast Surg. 2021;54(4):489-94.
10. Sabanciogullarindan S, Tunc S. Cicatricial eyebrow restoration using the follicular unit extraction technique. J Cosmet Dermatol. 2022;21(3):1098-1105.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}