


Elena de Lima Madureira; Dina Zylbersztejn; Alice Mota Buçard; David Rubem Azulay
Submitted on: 18/10/2022 Approved on: 24/07/202
Financial support: None.
Conflict of interest: None.
How to cite this article: Madureira EL, Zylbersztejn D, Buçard AM, Azulay DR. Impact of the COVID-19 pandemic on the epidemiological and clinicopathological profile of cases of primary cutaneous melanoma diagnosed at Instituto de Dermatologia Professor Rubem David Azulay. Surg Cosmet Dermatol. 2023;15:20230188.
SUMMARY: Melanoma is the main cause of death in dermatology (it is an aggressive type of skin cancer being one of the main causes of cancer death) due to its high metastatic power. When detected in early stages, its surgical treatment can be curative. When detected in more advanced stages, its prognosis is reserved and can be lethal. During the period of the COVID-19 pandemic, many medical activities were suspended. There are few data in the literature evaluating the impact of the pandemic on the evolution of patients with melanoma.
OBJECTIVES: This study aimed to evaluate the impact of the COVID-19 pandemic on the epidemiological, clinical and histopathological aspects of melanomas diagnosed at the Instituto de Dermatologia Professor Rubem David Azulay (IDPRDA).
METHODS: This is an observational, retrospective and unicentric study, where the requests and histopathological reports of skin biopsies performed at IDPRDA between January 2018 and December 2021 were reviewed and their epidemiological and clinicopathological aspects were subsequently evaluated.
RESULTS: A significantly lower incidence of melanoma diagnosis was not found during the pandemic years, but patients were diagnosed at more advanced stages of the disease, which shows a delay in diagnosis due to Covid-19.
Keywords: Melanoma; COVID-19; Pandemics.
Melanoma is a neoplasm of neuroectodermal origin formed from the malignant transformation of melanocytes. The skin is the most frequently involved primary site, although it can also occur in other locations, such as mucous membranes, ocular uveal tract, and leptomeninges.1,2,3 Its etiopathogenesis is multifactorial, involving genetic and environmental factors.
Although skin cancer is common in Brazil and accounts for around 30% of all malignant tumors registered in the country, melanoma represents only 4% of malignant neoplasms of the organ, and it is one of the most serious forms of skin cancer due to its high possibility of causing metastasis. 4,5
Melanoma is prevalent in patients with low skin phototypes. Its risk tends to increase with age, and the current average diagnosis is at 65 years of age, with no significant difference between the sexes. 1,3,6
Its diagnosis should be suspected in all pigmented lesions that present changes in color, size, or shape. Asymmetry, irregular edges, varied colors, diameter greater than 6 mm, and evolutionary changes in the characteristics of the lesion make up the acronym “ABCDE” which guides the detection of suspicious lesions and indicates the performance of a biopsy for diagnostic confirmation. 6,7
The most common histopathological subtype of cutaneous melanoma is superficial spreading melanoma, corresponding to 70% of cases, followed by the nodular type, comprising 15% to 30% of cases.8,9,10 The level of tumor invasion (Breslow index) is the primary independent prognostic factor, followed by the presence of ulceration and mitotic index, respectively.9,11 In this context, the timely identification of skin lesions suspected of melanoma, even in the early stages, and adequate diagnostic and therapeutic management are essential for the prognosis of melanoma.12
The COVID-19 outbreak caused thousands of deaths worldwide and was declared a pandemic by the World Health Organization (WHO) in March 2020. During this period, many medical and surgical activities were suspended. Furthermore, many patients stopped seeking health services for fear of contracting the disease. The probable delays in the diagnosis of melanoma caused by the pandemic may have had serious consequences for patient survival in addition to an increase in morbidity and mortality rates.13,14,15 There are few data in the literature assessing the consequences of the pandemic on melanoma. This study aims to evaluate the impact of the COVID-19 pandemic on the epidemiological and clinicopathological aspects of melanomas diagnosed at the Professor Rubem David Azulay Institute of Dermatology (IDPRDA).
It is an observational, retrospective, and single-center study conducted at Professor Rubem David Azulay Institute of Dermatology (IDPRDA) in the city of Rio de Janeiro.
We reviewed the files corresponding to the requests and histopathological reports of skin biopsies conducted at IDPRDA between January 2018 and December 2021. The study included all histopathological reports where melanoma was the final diagnostic conclusion. We excluded cases of nail melanoma, melanomas diagnosed in other services, and patients with not properly identified medical records.
Data collection was conducted using the protocol presented in Annex 1, based on the review of patients’ physical and/or electronic medical records, medical requests, and histopathological reports referring to all selected cases. The patients were distributed into three large groups, according to the year of melanoma diagnosis.
Finally, we identified 108 histopathological reports compatible with melanoma. Of these, 57 were diagnosed between 2018 and 2019 and allocated to the pre-pandemic group, 25 were diagnosed in 2020 and allocated to the pandemic year 1 group, and 26 were diagnosed in 2021 and allocated to the pandemic year 2 group.
The calculations presented in this study used the aid of the R 4.0.5 software (R Core Team, 2021), and, for statistical tests, a significance level of 5% was adopted. Comparison between groups was performed using the Fisher test, for variables with two categories, and the chi-square test, for variables with three or more categories.
The Research Ethics Committee of the Pontifical Catholic University of Rio de Janeiro (CEP PUC-Rio) approved the present study under ethical opinion number 05-2022.
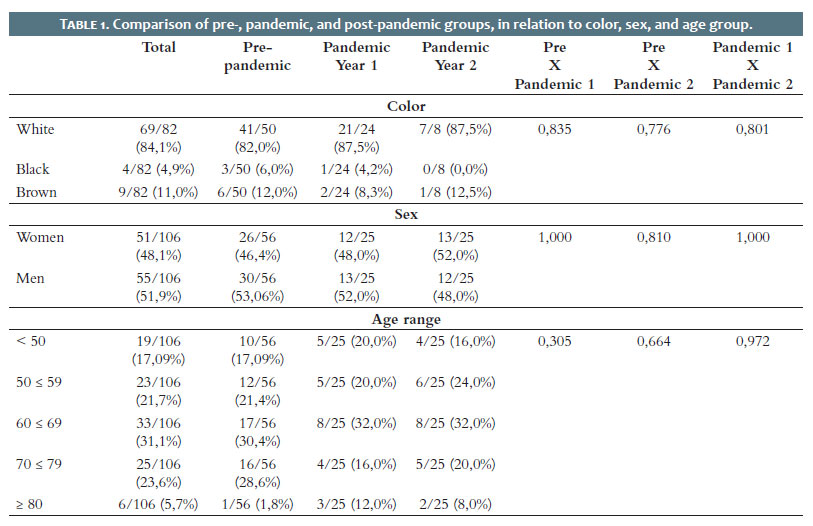
The 108 diagnosed cases corresponded to lesions from 106 patients: 55 men (51.9%) and 51 women (48.1%).
There were 69 white patients (84.1%), four black patients (4.9%), and nine brown patients (11%). Skin color was not reported in 24 patients.
The age of patients at the time of diagnosis ranged from 32 to 89 years.
The most affected age group was 60-69 years old in all study groups (Table 1).
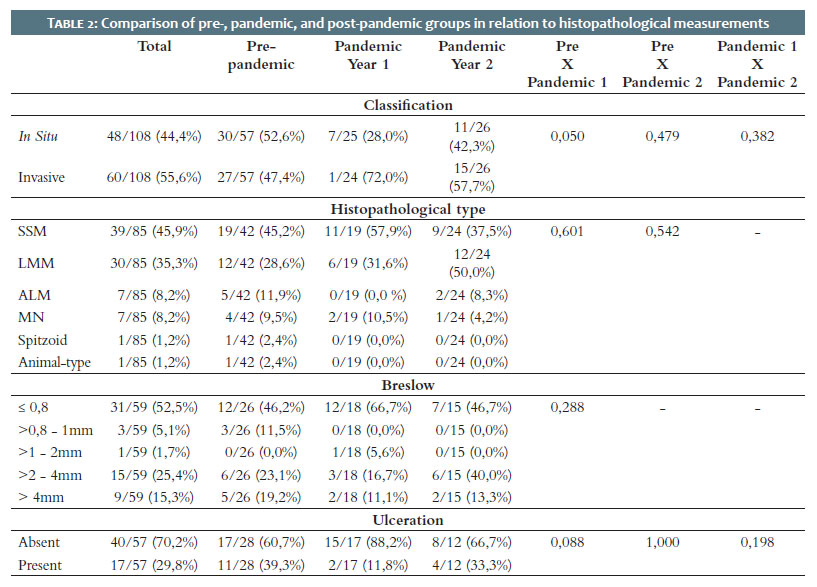
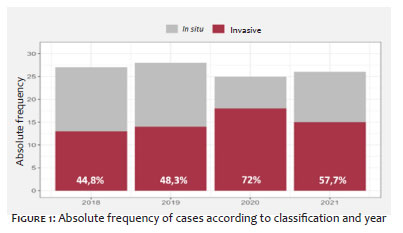
Of the 108 cases in the sample, 48 (44.4%) met diagnostic criteria for primary cutaneous melanoma in situ and 60 (55.6%) for primary invasive cutaneous melanoma (p-value 0.05). When we evaluated the different groups, we perceived that in the years before the pandemic, 52.6% of patients had an in situ tumor at the time of diagnosis. When we assessed patients diagnosed during the first year of the pandemic, we observed a change in this pattern: only 28% of melanomas were in situ at the time of diagnosis, while 72% were already invasive.
Regarding the histopathological subtype, 45.9% presented superficial spreading melanoma; 35.3%, lentigo maligna; 8.2%, acral lentiginous; 8.2%, nodular; 1.2%, spitzoid; and 1.2% had animal-type melanoma. The superficial spreading histopathological subtype was the most frequently found in all groups, except in the pandemic year 2 group, where the lentigo maligna melanoma subtype was the preponderant. We observed ulceration in 29.8% of the study cases: in the pre-pandemic group, 39.3% of patients presented ulceration; in the pandemic year 1 group, there were 11.8% of cases; and, in the pandemic year 2 group, there were 33.3% of cases.
Regarding the Breslow index, it was ≤0.8 mm in 52.5% of cases; >0.8 mm – 1 mm in 5.1% of cases; >1 mm – 2 mm in 1.7% of cases; >2 mm – 4 mm in 25.4% of cases; and >4 mm in 15.3% of cases. When we evaluated the different groups, we observed that, in the pre-pandemic period, 42.3% of patients had a Breslow index >1 mm. In the pandemic year 2 group, 53.3% of patients had a Breslow index >1 mm (Table 2).
Regarding the location of the tumor, the back was the most affected site with 25% of cases; followed by the upper limbs, with 20.4%; face, with 18.5%; acral region, chest, abdomen, and lower limbs, all with 8.3%; and, finally, the neck, responsible for only 2.8% of cases.
Concerning “ABCDE”, 75.9% of the cases in the study presented at least one indicator of the acronym (Table 3).
In March 2020, the World Health Organization (WHO) declared the COVID-19 outbreak a pandemic. During this period many medical and surgical activities had to be postponed or even suspended. The IDPRDA had to interrupt its activities for three months (20/03/2020 to 23/06/2020) when a lockdown was conducted in the city of Rio de Janeiro aiming to reduce the spread and cases of the disease. Furthermore, many patients stopped seeking health services for fear of contracting the virus. There is concern among healthcare professionals that the pandemic may have affected the incidence and early diagnosis of patients with malignant melanoma. 16,17
Melanoma is an aggressive type of skin cancer due to its high metastatic potential. Fortunately, most patients newly diagnosed with melanoma are at an early stage of the disease, and surgical excision is the treatment of choice, which is curative in most cases. When diagnosed in more advanced stages, it can be lethal, and therefore, early diagnosis is crucial for the survival of these patients. 18,19,20
Considering the sociodemographic variables, the characteristics of the patients were equivalent, that is, we found no significant difference between the groups. In agreement with the literature, the most affected patients were those with lower skin phototypes (84.1%).16 The most affected age group was 60-69 years old, representing 31.1% of patients. Also in agreement with the literature, differences regarding sex were not relevant in terms of incidence: 51.9% were men, while 48.1% were women.
We did not observe a significant drop in the incidence of melanoma diagnoses at our institution during the pandemic period. There were 29 cases diagnosed in 2018, 28 in 2019, 25 in 2020, and 26 in 2021. Regarding the severity of the tumor, when we compared the pre-pandemic group with the pandemic years 1 and 2 groups, we observed an increase in the diagnosis of more advanced tumors in the latter, a likely reflection of the pandemic and its consequent delay in diagnosing these patients. Figure 1 presents the classification frequencies for each year.
Regarding tumor severity, it is known that the most important prognostic factor for invasive melanomas is the Breslow index.1,21 When we assessed the collected data, we observed that, in the pre-pandemic group, 42.3% of invasive melanomas had a Breslow index >1 mm while, in the pandemic year 2 group, this value increases to 53.3%, which also reflects a likely diagnostic delay due to the pandemic (Figure 2).
The second most important prognostic factor for melanomas is ulceration.1,21 Many authors have described ulceration as the best indicator of the likelihood of lymph node involvement. In our study, ulceration was more common in patients diagnosed in the pre-pandemic period (39.3% in the pre-pandemic group, 11.8% in the pandemic year 1 group, and 33.3% in the pandemic year 2 group).
Regarding the histopathological subtype, the literature shows a predominance of the superficial spreading subtype, with a relative incidence among melanomas of 60-70% of cases, followed by the nodular melanoma subtype (15%), acral melanoma (10%) and, by last, the lentigo maligna subtype, with 5%.15,22,23 In our study, we also observed a predominance of the superficial spreading subtype (responsible for 45.9% of all cases). However, differing from the literature, the second prevalent subtype was lentigo maligna melanoma, responsible for 35.3% of cases.
Regarding clinical aspects, the back was the site most affected by melanoma (25% of cases), followed by the upper limbs (20.4%), face (18.5%), abdomen, chest, lower limbs and acral region (8.3% each), and neck (2.8%). The dorsal area was the most affected in the three study groups. However, we noted several diagnoses on the face in the pandemic year 2 group. We wonder if these patients observed themselves more during the period of seclusion or if their family members paid more attention to these patients.
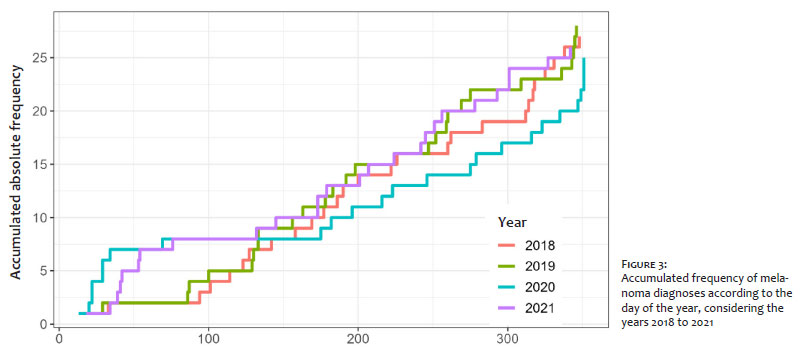
During the study, it was also possible to observe a greater frequency of diagnoses conducted in the first 100 days of the pandemic years. (Figure 3)
The greater demand for care in the first 100 days of 2020 can perhaps be explained by the fact that there are already rumors of COVID-19 in other countries and the possible onset of a global pandemic, which may have led to a greater need for health services before a possible lockdown. The greater demand for care in the first 100 days of 2021 could be explained by the start of vaccination in Rio de Janeiro and a more controlled pandemic scenario in which the end of the lockdown had already been decreed.
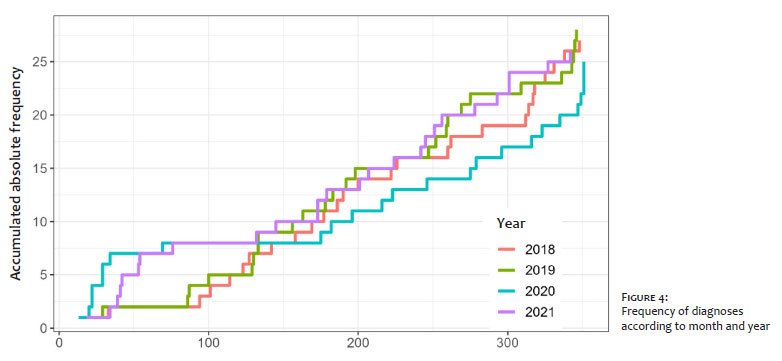
Figure 4 shows the absolute frequencies of diagnoses according to month and year. In this figure, it is possible to identify the closing date of the Service (03/20/2020), its reopening (06/23/2020), and the start of vaccination in RJ (02/17/2021).
We showed that there was no sociodemographic difference between the groups resulting from the pandemic.
We did not find a significantly lower incidence of melanoma diagnosis during the pandemic years. However, patients were diagnosed at more advanced stages of the disease, which shows a likely delay in diagnosis resulting from COVID-19.
In agreement with other studies, we found a predominance of the superficial spreading subtype in our Service. However, the second prevalent subtype was lentigo maligna instead of nodular melanoma, as the literature shows.
REFERENCES:
1. Azulay DR. Azulay Dermatologia. 8th ed. Rio de Janeiro: Guanabara Koogan; 2022.
2. Elder DE. Melanocytic tumours. In: ELDER DE. WHO Classification of skin tumours. France: IARC; 2017.
3. Garbe C, Bauer J. Melanoma. In: Bolognia JL, Schaffer JV, Cerroni L. Dermatology. 4th ed. United States of America: Elsevier; 2018.
4. Brandão FV, Pereira AFJR, Gontijo B, Bittencourt FV, et al. Aspectos epidemiológicos do melanoma em serviço de dermatologia de hospital universitário em um período de 20 anos. An Bras Dermatol. 2013;88(3):348-57.
5. Instituto Nacional do Câncer. Câncer de pele melanoma. Rio de Janeiro: INCA; 2021. Available from: https://www.inca.gov.br/tipos-de-cancer/cancer-de-pele- melanoma.
6. Almeida FA, Santos IDAO, Bakos L. Manual de recomendações em melanoma do GBM. Available from: https://visana.com.br/clientes/gbm/index.php/manual-de- recomendacoes/.
7. American Cancer Society. Cancer Facts & Figures 2020. Atlanta, Ga: American Cancer Society; 2020.
8. Ministério da Saúde (Brasil). Instituto Nacional de Câncer José Alencar Gomes da Silva (INCA). Coordenação de Prevenção e Vigilância. Estimativa 2018: Incidência de Câncer no Brasil. Rio de Janeiro: INCA; 2017. Available from: www.inca.gov.br.
9. Cabo HA. Color Atlas of Dermoscopy. New Delhi: Jaypee Brothers Medical Publishers; 2017.
10. Instituto Nacional do Câncer. Câncer de pele melanoma. Rio de Janeiro: INCA; 2021. Available from: https://www.inca.gov.br/tipos-de-cancer/cancer-de-pele- melanoma.
11. Elmas ÖF, Demirbas A, Düzayak S, Atasoy M, Türsen Ü, Lotti T. Melanoma and COVID-19: a narrative review focused on treatment. Dermatol Ther. 2020;33:e14101.
12. Martínez-Piva MM, Vacas AS, Rodríguez Kowalczuk MV, Gallo F, Rodrígues Vasconcelos M, Mazzuoccolo LD. Dermoscopy as a tool for estimating breslow thickness in melanoma. Actas Dermosifiliogr. 2021;112(5):434-40. English, Spanish. Epub 2020 Nov 28.
13. Baumann BC, MacArthur KM, Brewer JD, Mendenhall WM, Barker CA, Etzkorn JR, et al. Management of primary skin cancer during a pandemic: multidisciplinary recommendations. Cancer. 2020;126(17):3900-6.
14. Sociedade Brasileira de Dermatologia. Mais de 17 mil casos de câncer de pele deixaram de ser diagnosticados no auge da pandemia de COVID-19. Available from: sbd.org.br/mais-de-17-mil-casos-de-cancer-de-pele-deixaram-de-ser-diagnosticados-no-auge-da-pandemia-de-covid-19/
15. Gershenwald JE. Melanoma of the Skin. In: Amin MB. AJCC Cancer Staging Manual. 8th ed. United States of America: Springer; 2017.
16. Instituto Nacional do Câncer. Câncer de pele melanoma. Rio de Janeiro: INCA; 2021. Available from: https://www.inca.gov.br/tipos-de-cancer/cancer-de-pele- melanoma.
17. Instituto Nacional do Câncer. Câncer de pele melanoma. Rio de Janeiro: INCA; 2021. Available from: https://www.inca.gov.br/tipos-de-cancer/cancer-de-pele- melanoma.
18. Conic RZ, Cabrera CI, Khorana AA, Gastman BR. Determination of the impact of melanoma surgical timing on survival using the National Cancer Database. J Am Acad Dermatol. 2018;78(1):40-6.
19. Gershenwald JE. Melanoma of the Skin. In: Amin MB. AJCC Cancer Staging Manual. 8th ed. United States of America: Springer; 2017.
20. Gomolin T, Cline A, Handler MZ. The danger of neglecting melanoma during the COVID-19 pandemic. J Dermatolog Treat. 2020;29:1–8.
21. Ocanha-Xavier JP. Melanoma: características clínicas, evolutivas e histopatológicas de uma série de 136 casos. An Bras Dermatol. 2018;93(3):373-6.
22. Mitchell TC, Karakousis G, Schuchter L. Chapter 66: melanoma. In: Niederhuber JE, Armitage JO, Doroshow JH, Kastan MB, Tepper JE, eds. Abeloff’s Clinical Oncology. 6th ed. Philadelphia, Pa: Elsevier; 2020.
23. Naming the coronavirus disease (COVID-19) and the virus that causes it. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical- guidance/naming-the-coronavirus-disease-(covid-2019)-andthe-virus-that- causes-it. Accessed July 13, 2020.
Elena de Lima Madureira 0000-0001-5419-9201
Study design and planning; preparation and writing of the manuscript; collecting, analyzing and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Dina Zylbersztejn 0000-0001-6737-657X
Statistical analysis; approval of the final version of the manuscript; critical literature review; critical review of the manuscript.
Alice Mota Buçard 0009-0006-4189-0283
Author’s contribution: Approval of the final version of the manuscript; study design and planning; critical review of the manuscript.
David Rubem Azulay 0000-0003-4288-3692
Critical literature review; critical review of the manuscript.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}