


João Victor Bezerra; Luiza Vasconcelos-Schaefer
Submitted on: 01/05/2023
Approved on: 03/08/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Bezerra JV, Vasconcelos-Schaefer L. Persistent Intermittent Delayed Swelling (PIDS) caused by Hyaluronic Acid filler after five years: report of late complication. Surg Cosmet Dermatol. 2023;15:20230259.
Persistent Intermittent Delayed Swelling (PIDS) is an immune-mediated inflammatory reaction resulting from the interaction of immunological factors and the product's intrinsic characteristics. Such a reaction generally occurs after 30 days and persists while hyaluronic acid (HA) is in the area. We present through this case report a PIDS-type reaction that occurred five years after the injection of the product.
Keywords: Foreign body reaction; Dermal fillers; Hyaluronic acid
Persistent Intermittent Delayed Swelling (PIDS) occurs transiently, recurrently, and intermittently after filling with hyaluronic acid (HA), characterized by non-pitting and disseminated edema in the region where the product was applied, appearing after 30 days and persisting as long as there is HA on site.1 Ultrasound has proven to be a valuable tool for managing this complication.
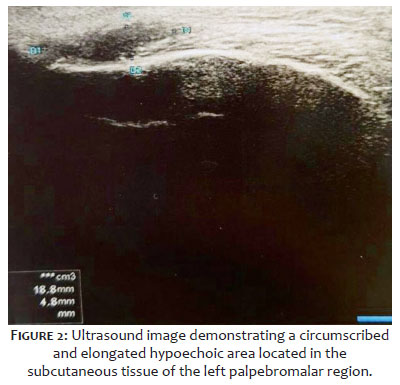
A 59-year-old woman reported the sudden onset of a painful and elevated area in the left palpebromalar transition region in the same place where hyaluronic acid filler was applied (hyaluronic acid 20 mg/ml) to correct deep dark circles, conducted five years ago with the same professional. She denied previous similar episodes and any other injectable procedure on the face. The patient also negated illness or vaccination in the last six months. On physical examination, she presented edema and erythema in the left palpebromalar region (Figure 1). As a diagnostic complement, we performed an ultrasound (US) of the area, demonstrating a hypoechogenic, circumscribed, and elongated formation located in the subcutaneous tissue, measuring 1.8 x 0.4 x 0.3 cm (estimated volume of 0.1 ml), compatible with exogenous material, in addition to vascular structures medial to the formation (Figure 2).
Due to reports of allergy to bee stings, treatment with hyaluronidase was contraindicated. We opted for a short, low-dose cycle (<1 mg/kg/day) of prednisone 60 mg/day for three days and 20 mg/day for another four days and light local massage. The patient evolved with significant improvement in edema and pain after the end of treatment (Figure 3), and she remained without new similar episodes after two years (bimonthly follow-up in the first six months and every six months thereafter).
Persistent Intermittent Delayed Swelling (PIDS) secondary to hyaluronic acid filling is an inflammatory reaction. Its mechanism is not yet fully understood, but there is increasing evidence of immunological interaction and intrinsic characteristics of the product used.2,3 It can be triggered by viral or bacterial infections and after vaccination.4,5,6 Several studies indicate complications similar to PIDS, but there is still no systematization defined by experts on adverse reactions to HA.
The use of ultrasound examinations has grown in Dermatology, being helpful for HA implantation and evaluation of complications, making it possible to determine the nature of the injected material, impairment of adjacent vascularization, and identification of inflammatory processes and/or necrosis. It can also be used for biopsies and guided injection of hyaluronidase and corticosteroids, with the advantage of being a non-invasive examination with no risk or discomfort for the patient.7,8 The common appearance of HA on US is of a well-defined oval formation and anechoic, similar to true cysts. In PIDS, HA is observed in the edematous area, with an increase in the thickness and echogenicity of the subdermal tissue, corresponding to panniculitis.7,8
The recommended procedures among specialists include hyaluronidase, systemic and intralesional corticosteroids, and antibiotic therapy (if associated biofilm is suspected), in addition to expectant management.9,10
Previous studies, lasting between two years11 and 68 months,12 reported episodes compatible with PIDS, with a single case of edema appearing after two months of treatment11 and 23 cases of nodules appearing between one and 13 months after filler.12 The present report demonstrated that such complication is possible while HA is in the tissue, requiring more long-term observational studies, in addition to active surveillance of injecting professionals regarding the possibility of this event.
João Victor Bezerra
ORCID: 0000-0002-7938-8794
Approval of the final version of the manuscript; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Luiza Vasconcelos-Schaefer
ORCID: 0000-0001-9837-9714
Approval of the final version of the manuscript; preparation and writing of the manuscript; effective participation in research guidance; critical literature review; critical review of the manuscript.
1. Cavallieri FA, Balassiano LKA, Bastos JT, Fontoura GHM, Almeida AT. Edema tardio intermitente e persistente ETIP: reação adversa tardia ao preenchedor de ácido hialurônico. Surg Cosmet Dermatol. 2017;9(3):218-22.
2. Alijotas-Reig J, Fernández-Figueras MT, Puig L. Inflammatory, imune-mediated adverse reactions related to soft tissue dermal fillers. Semin Arthritis Rheum. 2013;43(2):241-58.
3. Beleznay K, Carruthers JD, Carruthers A, Mummert ME, Humphrey S. Delayed-onset nodules secondary to a smooth cohesive 20 mg/mL hyaluronic acid filler: cause and management. Dermatol Surg. 2015;41(8):929-39.
4. Estébanez A, Pérez-Santiago L, Silva E, Guillen-Climent S, García-Vázquez A, Ramón MD. Cutaneous manifestations in COVID-19: a new contribution. J Eur Acad Dermatol Venereol. 2020;34(6):e250-1.
5. Ortigosa LCM, Lenzoni FC, Suárez MV, Duarte AA, Prestes-Carneiro LE. Hypersensitivity reaction to hyaluronic acid dermal filler after COVID-19 vaccination: a series of cases in São Paulo, Brazil. Int J Infect Dis. 2022;116:268-70.
6. Savva D, Battineni G, Amenta F, Nittari G. Hypersensitivity reaction to hyaluronic acid dermal filler after the Pfizer vaccination against SARS-CoV-2. Int J InfectDis. 2021;113(29):233-5.
7. Wortsman X, Wortsman J, Orlandi C, Gardenas G, Sazunic I, Jemec GBE. Ultrasound detection and identification of cosmetic fillers in the skin. J Eur Acad Dermatol Venereol. 2012;26(3):292-301.
8. Quezada-Gaón N, Wortsman X. Ultrasound-guided hyaluronidase injection in cosmetic complications. J Eur Acad Dermatol Venereol. 2016;30(10):e39-e40.
9. Urdiales-Gálvez F, Delgado NE, Figueiredo V, Lajo-Plaza JV, Mira M, Moreno A, et al. Treatment of soft tissue filler complications: expert consensus recommendations. Aesthet Plastic Surg. 2018;42(2):498-510.
10. Almeida AT, Banegas R, Boggio R, Bravo B, Braz A, Casabona G, et al. Diagnóstico e tratamento dos eventos adversos do ácido hialurônico: recomendações de consenso do painel de especialistas da América Latina. Surg Cosmet Dermatol. 2017;9(3):204-13.
11. Callan P, Goodman GJ, Carlisle I, Liew S, Muzikants P, Scamp T, et al. Efficacy and safety of a hyaluronic acid filler in subjects treated for correction of midface volume deficiency: a 24 month study. Clin Cosmet Investig Dermatol. 2013;6:81-9.
12. Beleznay K, Carruthers JD, Carruthers A, Mummert ME, Humphrey S. Delayed- onset nodules secondary to a smooth cohesive 20 mg/mL hyaluronic acid filler: cause and management. Dermatol Surg. 2015;41(8):929-39.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}