


Suellen Ramos de Oliveira1; Thiago Jeunon1; Carolina Fechine2
Submitted on: 27/04/2023
Approved on: 03/07/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Oliveira SR, Jeunon T, Fechine C. Pilomatrixoma of the scalp: peculiar presentation possibly related to topography. Surg Cosmet Dermatol. 2023;15:e20230257.
Pilomatrixoma is a benign tumor with differentiation to the hair matrix that can affect different regions of the skin. We report the case of a patient with an unusual presentation on the scalp, with warning signs for the possibility of a malignant variant of the tumor. We emphasize the importance of documenting atypical conditions that may permeate the practice of dermatologists and the need to rule out malignancies in the face of a change in the pattern of skin lesions, exulcerations, and bleeding, among other signs. The role of histopathology is fundamental for diagnostic definition and therapeutic management.
Keywords: Pilomatrixoma; Skin neoplasms; Hair diseases
Pilomatrixoma is a benign cutaneous neoplasm with differentiation to the hair matrix, also known as Malherbe's calcifying epithelioma. The primary locations are the face, neck, and upper limbs. However, it can be found less frequently in other body regions.1 Mucosal, palmar, and plantar regions are not affected.2 Generally, it appears in the first decades of life, being very common in the pediatric age group, when it is often mistaken with other skin disorders.1,3
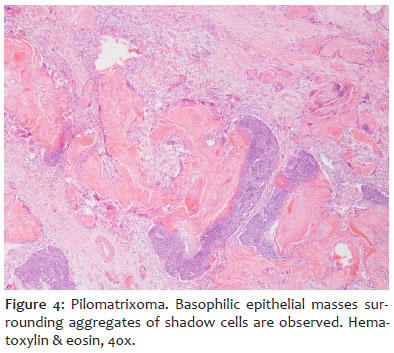
Clinically, although multiple nodules may be present, they are usually solitary, asymptomatic tumors with well-defined limits. The color of the skin over the neoplasm may be unchanged or vary in reddish or bluish tones.4,5 Diagnostic confirmation occurs through anatomopathological analysis, characterized by round or oval nodulation in the deep dermis, well-demarcated and circumscribed by a stromal capsule.2 Epithelial cells have medium vesicular nuclei and scant cytoplasm and are organized into irregular basophilic masses, accompanied by aggregates of keratinized cells known as "ghost cells" or "shadow cells".4
The main differential diagnoses are follicular cysts, foreign body reactions, adenopathies, histiocytosis, and other adnexal tumors.6 Pilomatrixoma treatment is conducted with complete surgical excision of the lesion, with recurrence occurring rarely.1
We report a case of a patient with an atypical presentation of pilomatrixoma on the scalp, with warning signs of the possibility of being a malignant variant of the tumor.
A 56-year-old man presented a nodular lesion on the scalp, in the parietal region, and hair loss for approximately one year. He reported a gradual lesion increase in this period, more pronounced in the last three months. The skin covering the lesion presented alopecia, erythema, erosion area, bleeding, and a central crust. It had a hard consistency on palpation but was mobile regarding deep planes, measuring approximately 3 cm (Figure 1).
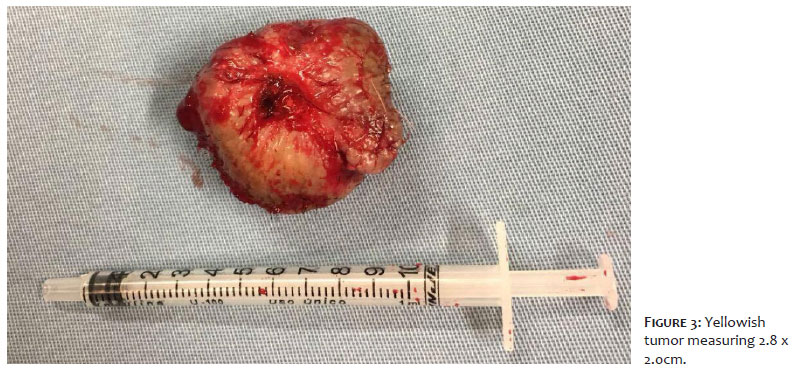
We performed an incisional biopsy, which indicated the diagnosis of pilomatrixoma. Subsequently, the patient underwent complete excision of the lesion under local anesthesia with closure using the O-Z flap technique (Figure 2). The tumor was yellowish and hardened, measuring 2.8 x 2.0 cm (Figure 3). The new histopathological examination confirmed the previous diagnosis with no evidence of malignancy (Figure 4).
Pilomatrixoma represents approximately 1% of benign skin tumors. In general, it progresses slowly and asymptomatically.7 The reported case demonstrates an atypical presentation of pilomatrixoma, with accelerated volume increase and local pain. Furthermore, the unusual location on the scalp, the patient's advanced age group, and clinical presentation with erosion and
this adnexal tumor, due to the highest concentration of follicular units per cm2.8
The malignant variant of pilomatrixoma is rare and receives different names, such as pilomatrix carcinoma, Malherbe's calcified epitheliocarcinoma, malignant pilomatricoma, or trichometric carcinoma. It is locally aggressive, has high recurrence rates, and presents metastases. Histological diagnosis is challenging, and sometimes cytological abnormalities are observed, such as cellular disorganization, with atypical and increased mitotic activity.1 Treatment in these cases is based on surgical excision associated with radiotherapy as a local adjuvant modality and, in the presence of metastases, evaluation of chemotherapy treatment.9 In our case, there was no sign of malignancy in the histopathological analysis of the tumor in its entirety.
In the literature, there are other cases where pilomatrixoma presents with an unusual manifestation, with an exophytic appearance, as occurred with our patient. Chen et al., in a clinicopathological analysis of 22 cases of pilomatrixoma, described clinical particularities according to the anatomical location of the lesions. Lesions found on the upper limbs were rigid, hardened, deep, and covered by apparently normal skin. The ones on the eyelids and face were blue-red and had a firm or elastic consistency. Lesions on the scalp were more prominent, as nodules and exophytic tumors were hardened and erythematous.10 The cases reported by Kondo et al. and Mendes et al. reproduced these characteristics, with pilomatrixoma lesions located on the bone plate of the skull, respectively, the supra-auricular and superciliary regions.1,7
We suggest that the site of pilomatrixoma on the skin, on the bone plate of the skull, would not allow tissue accommodation around an expansive nodule, causing the lesion to assume an exophytic and more erythematous character, raising the suspicion of a primary or metastatic neoplasm.
Pilomatrixoma can have an atypical clinical presentation depending on its location on the body, and the dermatologist must be aware of the clinical particularities of the lesion. Furthermore, we draw attention to the warning signs regarding the malignant variant of the tumor, which, despite being rare, cannot be ruled out without a histopathological study.
Suellen Ramos de Oliveira
ORCID: 0000-0002-6925-8785
Study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Thiago Jeunon
ORCID: 0000-0003-1750-438X
Author's contribution: Study design and planning; effective participation in research orientation; critical review of the manuscript.
Carolina Fechine
ORCID: 0000-0002-2873-8379
Author's contribution: Approval of the final version of the manuscript; effective participation in research orientation; critical review of the manuscript.
1. Mendes MH, Souza LP. Pilomatricoma recidivado em região superciliar esquerda: relato de caso. Arq Bras Oftalmol. 2009;72(3):380-3.
2. Benévolo AM, Loureiro AD, Oliveira DHS, Bernarde IC, Catelo Branco MDO. Pilomatricoma na região submandibular esquerda. Rev Bras Cir Cabeça Pescoço. 2010;39(2):157-9
3. Pirouzmanesh A, Reinisch JF, Gonzalez-Gomez I, Smith EM, Meara JG. Pilomatrixoma: a review of 346 cases. Plast Reconstr Surg. 2003;112(7):1784-9.
4. Greene RM, McGuff HS, Miller FR. Pilomatrixoma of the face: a benign skin appendage mimicking squamous cell carcinoma. Otolaryngol Head Neck Surg. 2004;130(4):483-5.
5. Fonseca RPL, Andrade FJS, Araujo IC, Silva FAF, Carvalho PNA. Pilomatricoma: epitelioma calcificado de Malherbe. Rev Bras Cir Plást . 2012;27(4):605-10.
6. Hernández-Núñez A, Nájera Botello L, Romero Maté A, Martínez-Sánchez C, Utrera Busquets M, Calderón Komáromy A, et al. Retrospective study of pilomatricoma: 261 tumors in 239 patients. Actas Dermosifiliogr. 2014;105(7):699-705.
7. Kondo RN, Pontello Junior R, Belinetti FM, Cilião C, Vasconcellos VRB, Grimaldi DM. Proliferating pilomatricoma - Case report. An Bras Dermatol. 2015;90(3 Suppl 1):94-6.
8. Han G, Kim AR, Song HJ, Oh CH, Jeon J. Updated view on epidemiology and clinical aspects of pilomatricoma in adults. Int J Dermatol. 2017;56(10):1032-6.
9. Sorin T, Eluecque H, Gauchotte G, De Runz A, Chassagne JF, Mansuy L, et al. Pilomatrix Carcinoma of the scalp. A case report and review of the literature. Ann Chir Plast Esthet. 2015;60(3):242-6.
10. Chen SY, Liu HT, Ho JC. [Pilomatricoma-a clinicopathological analysis of 22 cases, including 2 cases of bullous pilomatricoma]. Changgeng Yi Xue Za Zhi. 1991;14(2):106-10.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}