


Walter Refkalefsky Loureiro; Fernanda Araujo Santos
Submission on: 22/02/2023
Approved on: 20/04/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Loureiro WR, Santos FA. Small particle hyaluronic acid as a new adjuvant treatment option for atopic dermatitis. Surg Cosmet Dermatol. 2023;15:e20230229.
Atopic dermatitis (AD) is a chronic skin disease whose hallmark is a deficient skin barrier. Current treatment consists of restoring this barrier using emollients, reported corticosteroids, and systemic medications in severe cases. This study aimed to evaluate the subdermal hyaluronic acid (HA) injection to treat AD. We applied HA to plaques of atopic dermatitis, and there was a global improvement in the lesions and skin elasticity after two weeks. There was no complete regression of the plaques; however, HA can be proposed as an adjuvant treatment option for key areas.
Keywords: Hyaluronic acid; Dermatitis, Atopic; Therapeutics
Atopic dermatitis (AD) is a chronically relapsing skin disease that affects 2-8% of the adult population worldwide with significant impact on quality of life. The hallmark is a deficient skin barrier due to filaggrin mutations and abnormal lipid metabolism.1 It results in increased transepidermal water loss (TEWL), dehydration, and dry skin. Treatment consists of restoring the skin barrier with syndets, moisturizers, and management of eczema with topical corticosteroids, calcineurin inhibitors, and systemic medications in severe cases.
Small Particle Non-Animal Stabilized Hyaluronic Acid (SP-NASHA; Restylane Skinboosters Vital 20mg/mL and Vital Light 12mg/mL; Galderma Uppsala, Sweden) have been used for improving skin. Microdroplets of gel are injected into the dermis or subdermis with a needle or cannula to avoid visible or palpable products. It has been shown that treatment with SP-NASHA can improve skin hydration determined by corneometry, especially in subjects presenting with dehydrated skin at the baseline. Injections don't increase TEWL and may decrease it in areas such as the hands, retaining more moisture in the tissue. Data suggests that SP-NASHA may hydrate and also reverse a damaged skin barrier. Skin elasticity is improved after three months of treatment as measured by a cutometer. Long-term efficacy has been documented up to 24 weeks after treatment.2,3,4
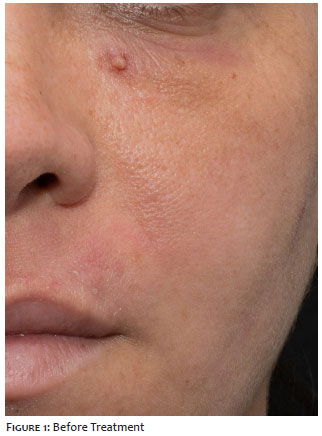
The author reports the treatment of a 36-year-old woman with severe adult atopic dermatitis in regular use of syndet gels, moisturizers, and occasional topical corticosteroids with insufficient control. The patient had criteria for systemic treatment, but she was not inclined to it at the time. She presented recurrent eczema lesions throughout the body but complained particularly of periorbital and perioral regions, cheeks, neck, and inner proximal thigh (Figures 1 and 3). We injected The SP-NASHA subdermally in linear threads with a 25 G cannula, leaving small depots of approximately 10 µL (1 SmartClickTM) per 0.5 cm in a retrograde injection. Each 1 mL syringe was dispensed throughout an area of a hand palm except fingers. The periorbital area was treated with 0.5 mL on each side. Cheeks (2 mL) and proximal inner thigh (2 mL) were treated with Restylane Vital, while periorbital area (1 mL) and neck (2 mL) received Restylane Vital Light. The patient returned after two weeks for a second session of another 1 mL in each area of the same previous product. Total amounts were 2 mL for periorbital and 3mL for cheeks, neck and thigh.
She kept the same daily routine. The patient returned two weeks after the treatment with improved lesions in all areas, especially neck and thigh (Figures 2 and 4). She referred to an episode of mild and brief worsening after exposure to dust (home renewal), but much less intense than expected from personal previous experience. She reported an improvement in neck skin elasticity.
SP-NASHA will not cure adult AD. However, it may be a new option for improving quality of life and skin in localized areas. To our knowledge, this is the first published report of injectable HA as a treatment modality for adult AD. Controlled studies with longer follow-ups are required to establish treatment protocols and achieve best clinical outcomes.
Walter Refkalefsky Loureiro
ORCID: 0000-0002-4957-9215
Approval of the final version of the manuscript; Study design and planning; Effective participation in research orientation; Critical literature review; Manuscript critical review.
Fernanda Araujo Santos
ORCID: 0000-0003-4895-9168
Statistical analysis; Data collection, analysis and interpretation; Preparation and writing of the manuscript; Intellectual participation in propaedeutic and/or therapeutic management of studied cases.
1. Wollenberg A, Barbarot S, Bieber T, Christen-Zaech S, Deleuran M, Fink-Wagner A, et al. Consensus-based European guidelines for treatment of atopic eczema (atopic dermatitis) in adults and children: part I. J Eur Acad Dermatol Venereol. 2018;32(5):657-82.
2. Nikolis A, Enright KM. Evaluating the role of small particle hyaluronic acid fillers using micro-droplet technique in the face, neck and hands: a retrospective chart review. Clin Cosmet Investig Dermatol. 2018;11:467-75.
3. Wu Y, Tian Y, Xu J, Zhong S, Wang R, Wu W. A randomized study showing improved skin quality and aesthetic appearance of dorsal hands after hyaluronic acid gel treatment in a Chinese population. J Cosmet Dermatol. 2020;19(7):1627-35.
4. Ayatollahi A, Firooz A, Samadi A. Evaluation of safety and efficacy of booster injections of hyaluronic acid in improving the facial skin quality. J Cosmet Dermatol. 2020;19(9):2267-72.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}