


Daniela de Cássia Sampaio Miranda; Luísa Fernandes Rivelli Cardoso; Giovanni Indelicato Milano; Raissa Soares Neves da Costa; Luiza Laborne Sousa Pinto Kalil
Submitted on: 06/02/2023
Approved on: 20/04/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Miranda DCS, Cardoso LFR, Milano GI, Costa RSN, Kalil LLSP. Case report: Granuloma after infection of commercial hyaluronic acid serum. Surg Cosmet Dermatol. 2023;15:e20230224.
Foreign body granuloma can occur after injection of filling substances into the dermis. We report a case of a 35-year-old woman who performed a self-injectable injection of a commercial serum for exclusively topical use containing hyaluronic acid in the region of the dark circles for aesthetic reasons. After the procedure, she presented a nodule in the lower right eyelid, which she judged to be an accumulation of product. Then she injected betamethasone + hyaluronidase ointment (Postec®), evolving into a foreign body granuloma.
Keywords: Granuloma; Dermal fillers; Hyaluronic acid
Foreign body granuloma is a chronic inflammatory reaction due to foreign material in the organism or material from the organism itself in an ectopic location, composed mainly of macrophages and multinucleated giant cells.1
It can occur after the injection of fillers into the dermis, presenting several clinical and histological characteristics, depending on the type of material applied. It is a non-allergic reaction that occurs between 6 and 24 months after injections.1
Clinically, foreign body granulomas consist of papules, nodules, tumors, and/or fistulas located at the site where the foreign body is, presenting a clinical picture of prolonged evolution. The severity of foreign body granuloma can be classified into four degrees according to the types and number of cells present, ranging from 0, which corresponds to the absence of visible reaction, to 4, which would be encapsulated granuloma with foreign body reaction.2
According to Lee and Kim's systematic review, the factors that affect the formation of granulomas caused by dermal fillers are injected volume, repeated injections, impurities, particle size, surface and charge, and hydrophilicity. Among these factors, the surface of the particles and the presence of impurities stood out as particularly relevant.2
A 35-year-old woman from Belo Horizonte reported that, on May 21, she self-applied at home a commercial serum for topical use containing hyaluronic acid through intradermal injection in the dark circles area for aesthetic reasons. After the injection, she noticed a small nodule on the lower right eyelid in its most lateral portion, which she thought was an accumulation of product. Then, she injected betamethasone + hyaluronidase ointment (Postec®), available for topical use. About a week after product inoculation the lower right eyelid showed significant erythema and hardened nodules (Figure 1).
After the cutaneous manifestation, she used several topical medications on her own, such as dexamethasone, hydrocortisone, desoxymethasone + neomycin sulfate (Esperson® N), zinc bacitracin + neomycin sulfate (Nebacetin®), mupirocin, mucopolysaccharide polysulfate (Topcoid gel®), and mometasone. She also used systemic medications such as sulfamethoxazole + trimethoprim (400 mg + 80 mg/cp) twice daily for ten days and prednisone 40 mg daily for 30 days on July 21.
The patient had chronic myeloid leukemia as a comorbidity, and she was followed up by the Hematology Department of the same hospital. She was using nilotinib 400 mg twice daily, fluoxetine 20 mg daily, and clonazepam 1 mg daily. She had no history of drug allergies.
The primary diagnostic hypothesis was foreign body granuloma, but the hypothesis of atypical mycobacteriosis was also raised, mainly because it is a non-sterile product.
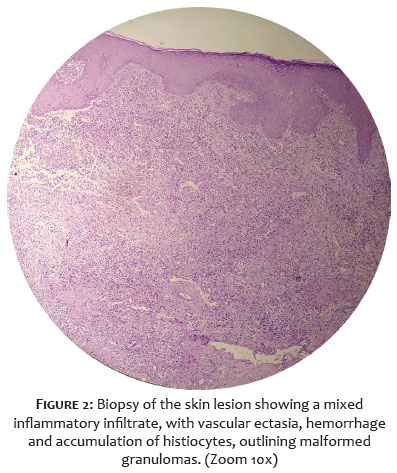
We performed a skin lesion biopsy with anatomopathological examination, which showed a mixed inflammatory infiltrate with vascular ectasia, hemorrhage, and accumulation of histiocytes, outlining malformed granulomas (Figure 2). Part of the material was sent for culture without the growth of mycobacteria.
We started an infiltration of triamcinolone 20 mg/ml diluted 1:4 in the region on November 21. We performed four sessions (Figure 3) and four spindle surgeries to excise some nodules that bothered the patient aesthetically (Figure 4). She is still under follow-up, showing a good response.
The first-line therapy for foreign body granulomas caused by fillers is the intralesional injection of corticosteroids as soon as possible.2 It is preferable to inject a high triamcinolone dose (e.g. , 40 mg) mixed with lidocaine (1:1 dilution) to prevent recurrence. Betamethasone or methylprednisolone can also be used without previous dilution.3 Local injection of corticosteroids interferes with the activities of fibroblasts, macrophages, giant cells, and collagen synthesis. There are many reports of success in the treatment of foreign body granulomas caused by Artecoll, hyaluronic acids, and Matridex, using intralesional steroid injections.2 It must be injected strictly into the nodule, holding it between two fingers. Strong resistance to the needle should be felt. Surgical excision may not be necessary if this therapy starts early and aggressively.3
Two to five sessions of intralesional corticosteroids at three-week intervals are suggested. If there is no improvement after two to four weeks, the dose should be doubled. A 0.5 mL or 1 mL insulin syringe with a 30-gauge needle is recommended for intralesional injections. A smaller diameter syringe allows granuloma resistance to be detected, which helps prevent corticosteroid-induced dermal atrophy.3
Intralesional 5-fluorouracil, an antimitotic agent, can work successfully in this type of granuloma, alone or combined with corticosteroids. The association between 5-fluorouracil and betamethasone seems to have a more potent anti-inflammatory effect 3 and a lower risk of atrophy than intralesional corticosteroids alone.3,4
Bleomycin, from experience with keloids and hypertrophic scars, may also work on granulomas. Systemic corticosteroids should be used for recurrent granulomas. Doses should be higher than those used for local injections. Oral prednisone (30 to 60 mg/day) is recommended to prevent recurrence of granulomas.3
Minocycline alone or combined with oral or intralesional corticosteroids is indicated for generalized inflammatory granulomas. It has anti-inflammatory, immunomodulatory, and antigranulomatous properties. Additionally, the literature has reported systemic treatment of foreign body granulomas with allopurinol, colchicine, and cyclosporine.2
There is also the option of using lasers. Small non-inflammatory granulomas responded well to long-pulse 532 nm lasers. Larger inflammatory granulomas have shown favorable responses to 1064 nm long pulse lasers.3
Intense pulsed light can treat the bluish discoloration of some superficial sclerosing foreign body granulomas effectively. Four to five sessions can block neovascularization and soften and shrink the underlying granuloma, likely reducing the blood supply.3
Excision of foreign body granulomas is not a first-choice therapy because complete removal of a granuloma is impossible in many cases. There may be complications such as abscess or fistula formation after surgery on granulomas that are induced by silicone fluid or acrylamide gel. In the case of an obvious sterile abscess, incision, and drainage are effective treatments.2
The reported case demonstrates the trivialization of cosmiatry in the current Brazilian scenario since even topical products are being self-applied for aesthetic purposes.
Foreign body granulomas can be effectively treated with intralesional corticosteroid injections. However, the correct early diagnosis is essential due to the rapid introduction of adequate therapy for a better response and exclusion of differential diagnoses such as atypical mycobacteriosis.
Even in cases where intralesional corticosteroid therapy may not be completely effective, its combined use with other treatments may reduce scarring, erythema, and edema, often allowing a surgical approach with less chance of complications.
Usually foreign body nodules and granulomas with little capsule formation and little tissue ingrowth - such as cystic granulomas, which may occur after injection of collagen or hyaluronic acid, or compacted nodules of calcium hydroxyapatite (Radiesse®), silicone, and polyacrylamides - do not react to corticosteroids or intralesional antimitotic drugs.
In such cases, drainage or surgical removal, especially of the labia, are probably the methods of choice.3
Daniela de Cássia Sampaio Miranda
ORCID: 0000-0002-6660-0530
Study design and planning; preparation and writing of the manuscript; effective participation in research orientation; intellectual participation in propedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Luísa Fernandes Rivelli Cardoso
ORCID: 0000-0002-8757-2866
Approval of the final version of the manuscript; preparation and writing of the manuscript; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Giovanni Indelicato Milano
ORCID: 0000-0002-7149-3194
Author's contribution: Approval of the final version of the manuscript; preparation and writing of the manuscript; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Raissa Soares Neves da Costa
ORCID: 0000-0001-5127-9986
Author's contribution: Intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Luiza Laborne Sousa Pinto Kalil
ORCID: 0000-0002-6069-5743
Author's contribution: Approval of the final version of the manuscript; preparation and writing of the manuscript; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
1. Belda W Jr, Chiacchio ND, Criado PR. Tratado de Dermatologia – volume 2. 3rd ed. São Paulo: Atheneu; 2018.
2. Lee JM, Kim YJ. Foreign body granulomas after the use of dermal fillers: pathophysiology, clinical appearance, histologic features and treatment. Arch Plast Surg. 2015;42(2):232-9.
3. Lemperle G, Gauthier-Hazan N. Foreign body granulomas after all injectable dermal fillers: part 2. Treatment options. Plast Reconstr Surg. 2009;123(6):1864-73.
4. Lemperle G, Rullan PP, Gauthier-Hazan N. Avoiding and treating dermal filler complications. Plast Reconstr Surg. 2006;118(3 Suppl):92S-107S.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}