


Matheus de Souza Moraes; Erica Pontes Pereira Ferreira
Submitted on: 15/03/2023
Approved on: 20/08/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Moraes MS, Ferreira EPP. Body photography in the diagnosis of melanoma: an integrative review. Surg Cosmet Dermatol. 2023;15:e20230238.
This integrative review included 22 studies aiming to identify the main conclusions regarding the use of total body photography for the diagnosis of melanoma. Thus, it demonstrated that the method could help in the early detection of melanoma, reducing unnecessary biopsies, identifying melanomas from new lesions, improving patient survival, and decreasing patient anxiety. However, it can be a high-cost method. Therefore, total body photography is a proficient tool in facilitating the monitoring and diagnosis of melanoma in patients at a certain risk.
Keywords: Melanoma; Diagnosis; Dermoscopy
Non-melanoma skin cancer has the highest incidence of cancer in Brazil. Data from the National Cancer Institute (INCA) demonstrated that, in 2020, the estimated incidence of this disease in the population was 176,940 new cases. Meanwhile, melanoma skin cancer had an estimated occurrence of 8,450 new cases in the same year. Although the percentage of cases of the latter is less than 5% of the total number of cutaneous neoplasms, its mortality reaches 43% compared to the same diseases.1
Despite the high incidence, the lesions are easy to diagnose, and the cure prognosis is higher than 95% when these lesions are identified and treated early.2 There is no cure for advanced cutaneous melanoma, so diagnosis and excision before advanced development are preferable. Thus, tools to assist dermatological examination with the naked eye have been developed, increasing sensitivity in detecting melanocytic lesions.3
Kopf and Slue at New York University first used total body photography (TBP) in 1988.3 The technique consists of taking photographic records that document injuries and provide a point of support for monitoring patients over time. The great advantage of this method is the possibility of identifying melanomas from new lesions.4
Typically, TBP applies to patients with multiple lesions or extensive or atypical nevi, aiming to diagnose melanomas early.5 Furthermore, this approach makes it possible to reduce the excision of benign lesions as the detection of increasingly thinner skin cancers increases, which routine dermatological examinations may not diagnose.6 Lesion Asymmetry, Border irregularity, Color variation, and Diameter greater than 6 mm comprise the ABCD of melanoma clinical diagnosis.2
TBP can occur alone or in combination with other diagnostic tools, such as sequential digital dermoscopy (SDD), which consists of recording and storing high-definition images of lesions with the highest suspicion of malignancy. This combination benefits patients more likely to develop melanoma (Fink & Haenssle, 2016). When the TBP is digitized, it is called TBDP ("Total Body Digital Photography").7, 8
In addition to the clinical benefits, TBP positively interferes with the mental health status of patients who undergo it, especially those with a personal history of melanoma.8 Therefore, this review aims to identify the main conclusions regarding the use of total body photography, isolated or not, for melanoma diagnosis.
It is a qualitative study through an integrative literature review. We used the National Library of Medicine (PubMed), Virtual Health Library (VHL), and Scientific Electronic Library Online (SciELO) databases. The chosen descriptors, intermediated by the Boolean operator "AND" to search for articles on the platforms were "melanoma", "total body photography", and "diagnosis". We found only the first and the last in the Health Sciences Descriptors (DeCS).
We conducted the literature review following the steps: establishment of the theme; definition of eligibility parameters; definition of inclusion and exclusion criteria; verification of publications in databases; examination of the information found; analysis of the studies and presentation of the results.9 Original articles in the experimental scope (clinical trials, randomized or non-randomized) and observational studies (cohort studies and case reports) were included in this study without a time frame. Articles relating to the topic, with unrelated descriptors, literature review-type, and duplicate papers were excluded.
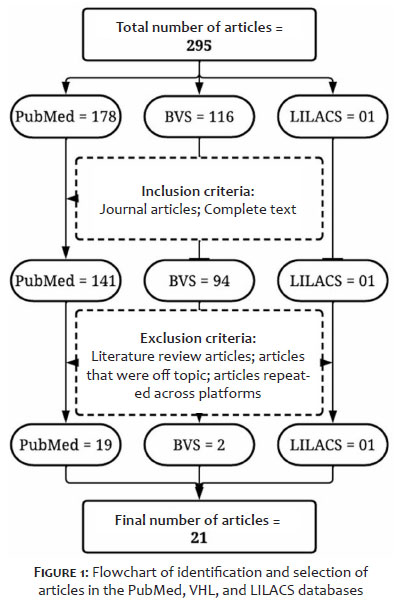
Initially, the search resulted in a total of 295 articles, 178 from PubMed, 116 from VHL, and 01 from Scielo. After applying the inclusion and exclusion criteria, we selected 22 articles: 19 from PubMed, 02 from VHL, and 01 from Scielo (Figure 1).
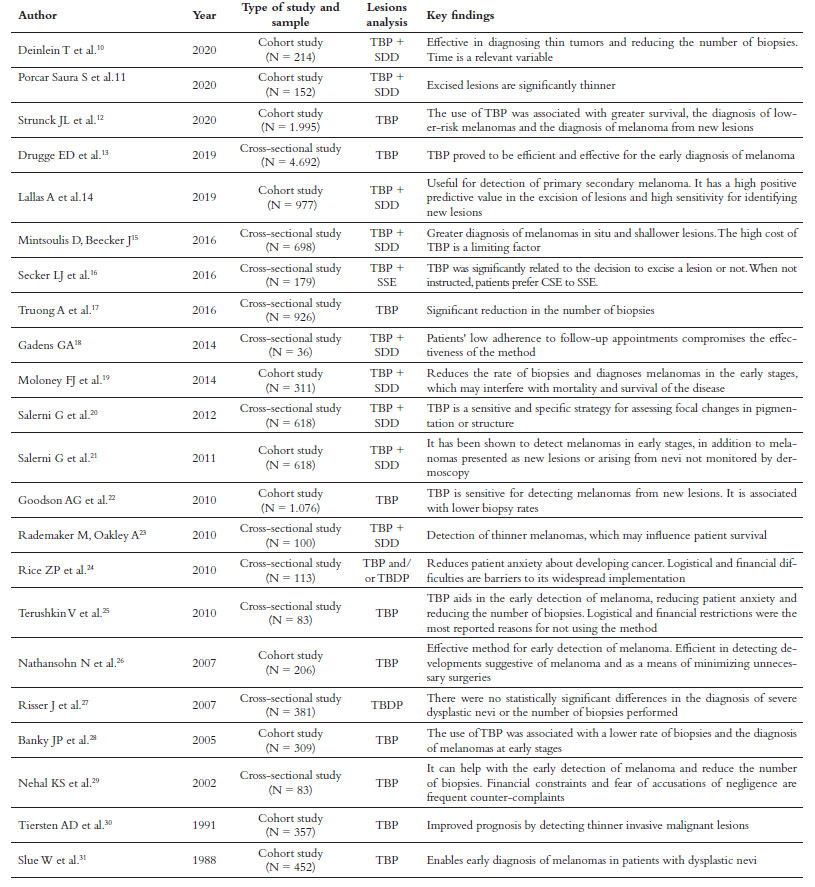
Among the 22 articles selected, half were cross-sectional studies, and the other half were cohort studies (Table 1). Of the total, 17 articles exclusively reported benefits when using TBP, associated or not with other methods, in the diagnosis of melanoma. On the other hand, four papers registered positive and negative points about using the tool, and only one article addressed the challenges of its use. Half of the articles addressed TBP as the only diagnostic tool; the other half associated TBP with digital Dermoscopy.
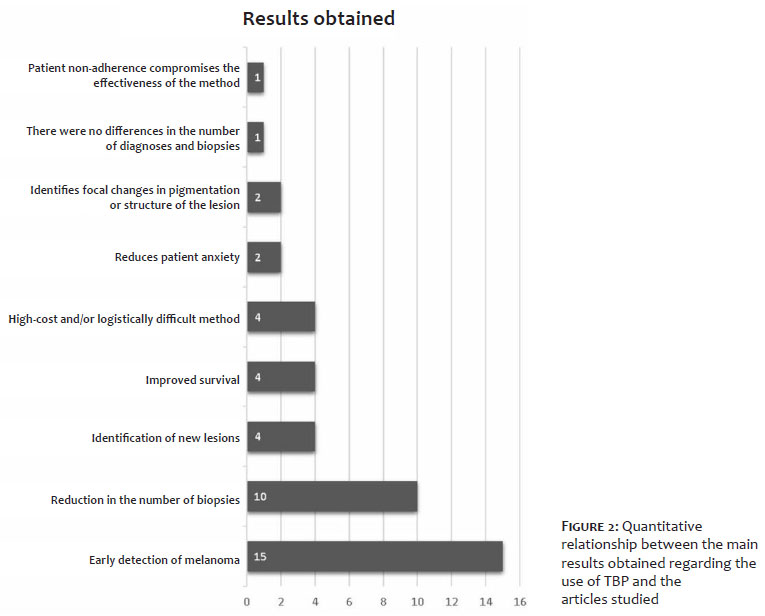
Regarding the main results, skin cancer early detection, reduced number of biopsies, improved survival, and new dysplastic lesions identification were the most mentioned benefits. On the other hand, the high cost of the method is considered an obstacle to its implementation, in addition to the low adherence of patients to monitoring. Figure 2 demonstrates the quantitative relationship between the main results obtained and the articles studied.
TBP is a method that has been widespread and allows for more careful monitoring of patients at high risk of developing melanoma.32 The results found in this study demonstrated that TBP is associated with early detection of these malignant lesions. This statement was reproduced in the study by Feit et al. (2004), conducted with 12 patients selected from a group of 576 people registered at the Dermatology Outpatient Clinic of the Memorial Sloan Kettering Cancer Center in New York (USA), where only one of 27 melanomas diagnosed through this procedure had thickness higher than 1 mm.33
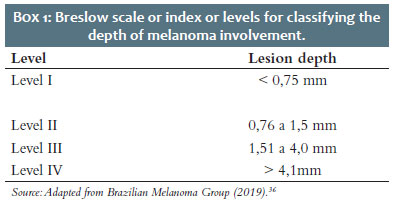
The Breslow scale or index (Box 1) is widely used in Dermatopathology to classify the depth of lesions: the more superficial, the better the prognosis.34 In cases of melanoma diagnosed using TBP, the significantly thinner depth impacts on the five-year survival rate of 95%.33 In contrast, a study with 926 patients carried out by Truong et al. (2016), comparing data from patients with melanoma before and after the implementation of the TBP, demonstrated that the variation in depth on the Breslow scale of patients without photographic monitoring was 0.2 mm to 3.0 mm (compared to 0.11 mm to 2.1 mm using the technique), corroborating the importance of the method.17 Thus, TBP can help in the early detection of melanoma and influence the prognosis of these patients.35
Another benefit was the reduction in biopsies in patients monitored by the studied tool. Goodson et al. (2010) report in their study that, of the 275 biopsies performed, 61% were a consequence of the use of TBP, detecting 12 melanomas, that is, the use of body photography increases the precision when performing biopsies.22 Furthermore, a complementary study by Truong et al. (2016) revealed that the average number of excisions per patient before TBP was 5.92. However, after its implementation, this average dropped to 1.56 biopsies per person, detecting 93 melanomas in 589 patients.17
In contrast, analysis of patient data between 1998 and 2003 by Risser et al. (2007) did not find statistically significant differences in the number of severe dysplastic nevi diagnosed and biopsies performed between patients under surveillance for TBP and patients monitored without this parameter. In this study, the average number of biopsies per patient biopsied and photographed was 0.8, while the average number of individuals biopsied and without this follow-up was 0.82.27 These results do not negate the need for new studies.
The retrospective cohort by Feit et al. (2004), with 576 patients observed periodically with standardized photographic records, indicated the diagnosis of 27 melanomas. Of this total number of lesions, 74% were identified due to the changes observed in their structure, both in the skin self-examination by the patient and in the dermatological examination by a doctor. Furthermore, 19% of the 27 melanomas represented new lesions not identified at the first consultation, information that exposed the recognition of new lesions as an essential part of melanocytic skin cancer diagnosis.33
Although it makes it possible to identify changes in the lesion structure and the emergence of new lesions, the research by Kelly et al. (1997), comprising 278 patients in a private dermatology service, highlighted the economic importance of TBP in health services. After 42 months of follow-up, 20 melanomas were diagnosed in 16 patients generating a cost of R$ 5,583.00 per melanoma using photographic records. Conversely, it proved that the prophylactic excisions necessary for the same prevention effect, without TBP, would result in an expense of R$ 395,038.00 for each melanoma since, of the 20 lesions, only three were pre-existing. Therefore, photographic monitoring of patients with many atypical pigmented lesions provided information on the stability of most lesions and avoided unnecessary biopsies.37
Regarding the applicability of the tool, Rice et al. (2010) report in their study with accredited Dermatology departments in the United States that among the obstacles to the use of TBP are mainly financial and logistical issues since the choice of how to take and record the photographs can affect the final cost. Even in a rich nation, the reimbursement rate offered by public health insurance in 2008 was between 20% and 30%, which may discourage the use of this technology. Furthermore, dermatologists who chose to adhere to the photographic record argued that it is a safety measure for patients in cases of medical error.24
The results of studies by Nehal et al. (2002) and Terushkin et al. (2010) reaffirm TBP as an effective tool in the early diagnosis of melanoma, as shown by Feit et al. (2004), as well as the identification of new lesions and the reduction in the number of unnecessary biopsies, outcomes also found by Kelly et al. (1997). At the same time, these authors highlight the advantage of reducing the patients' psychological stress due to their high risk of developing melanoma. The TBP offers a parameter to the skin examination and, therefore, reduces anxiety about changes in lesions.29, 25, 33, 37
Total body photography represents the advancement of technology associated with healthcare techniques and is a proficient tool in facilitating the monitoring and diagnosis of melanoma in patients at certain risks. Therefore, its access must be democratized through specialized centers with professionals in continued training since mortality from this type of skin cancer is statistically significant.
The biggest challenge for the widespread dissemination of the technique is its high cost, which would depend on the financial capacity of the Public Healthcare System (Sistema Único de Saúde - SUS). As an alternative, agreements could be signed between public bodies and private health systems, encouraging national research focused on health technologies. Finally, new research must be conducted to assess the technique within the dynamics of the national territory.
Matheus de Souza Moraes
ORCID: 0000-0003-4140-6915
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Erica Pontes Pereira Ferreira
ORCID: 0000-0002-9543-464x
Approval of the final version of the manuscript; effective participation in research guidance; critical review of the manuscript.
1. Instituto Nacional de Câncer. Plataforma INCA. Estimativas dos casos novos. Brasil: INCA, departamento científico; 2022. Disponível em: https://www.inca.gov.br/estimativa/estado-capital/brasil
2. Dimatos DC, Duarte FO, Machado RS, Vieira JV, Vasconcellos ZAA, Bins-ely J, et al. Skin melanoma in Brazil. Arq Catarin Med. 2009;38(1):14-9.
3. Wang SQ, Hashemi P. Noninvasive imaging technologies in the diagnosis of melanoma. Semin Cutan Med Surg. 2010;29(3):174-84.
4. Young AT, Vora NB, Cortez J, Tam A, Yeniay Y, Afifi L, et al. The role of technology in melanoma screening and diagnosis. Pigment Cell Melanoma Res. 2021;34(2):288-300.
5. Fried L, Tan A, Bajaj S, Liebman TN, Polsky D, Stein JA. Technological advances for the detection of melanoma: advances in diagnostic techniques. J Am Acad Dermatol. 2020;83(4):983-92.
6. Menzies SW. Cutaneous melanoma: making a clinical diagnosis, present and future. Dermatol Ther. 2006;19(1):32-9.
7. Fink C, Haenssle HA. Strategien zur nichtinvasiven siagnostik des melanoms [strategies for the noninvasive diagnosis of melanoma]. Hautarzt. 2016;67(7):519-28.
8. Moye MS, King SM, Rice ZP, DeLong LK, Seidler AM, Veledar E, et al. Effects of total-body digital photography on cancer worry in patients with atypical mole syndrome. JAMA Dermatol. 2015;151(2):137-43.
9. Pereira AS, Shitsuka DM, Parreira FJ, Shitsuka R. Metodologia da pesquisa científica. Santa Maria: UFSM; 2018. Disponível em: http://repositorio.ufsm.br/handle/1/15824
10. Deinlein T, Michor C, Hofmann-Wellenhof R, Schimid-Zalaudek K, Fink-Puches R. The importance of total-body photography and sequential digital dermatoscopy for monitoring patients at increased melanoma risk. J Dtsch Dermatol Ges. 2020;18(7):692-7.
11. Porcar Saura S, March-Rodríguez A, Pujol RM, Segura Tigell S. Two-step digital follow-up of patients at high risk for melanoma: a retrospective analysis of 152 patients. Actas Dermosifiliogr. 2021;112(3):250-6.
12. Strunck JL, Smart TC, Boucher KM, Secrest AM, Grossman D. Improved melanoma outcomes and survival in patients monitored by total body photography: a natural experiment. J Dermatol. 2020;47(4):342-7.
13. Drugge ED, Okundaye OI, Sarac RM, Drugge RJ. Melanoma screening using patient self-assessed risk and total body photography. Dermatol Online J. 2019;25(7):13030 /qt33h4r9bk.
14. Lallas A, Apalla Z, Kyrgidis A, Papageorgiou C, Boukovinas I, Bobos M, et al. Second primary melanomas in a cohort of 977 melanoma patients within the first 5 years of monitoring. J Am Acad Dermatol. 2020 ;82(2):398-406.
15. Mintsoulis D, Beecker J. Digital dermoscopy photographs outperform handheld dermoscopy in melanoma diagnosis. J Cutan Med Surg. 2016;20(6):602-5.
16. Secker LJ, Bergman W, Kukutsch NA. Total body photography as an aid to skin self-examination: a patient's perspective. Acta Derm Venereol. 2016;96(2):186- 90.
17. Truong A, Strazzulla L, March J, Boucher KM, Nelson KC, Kim CC, et al. Reduction in nevus biopsies in patients monitored by total body photography. J Am Acad Dermatol. 2016;75(1):135-43.
18. Gadens GA. Lack of compliance: a challenge for digital dermoscopy follow-up. An Bras Dermatol. 2014;89(2):242-4.
19. Moloney FJ, Guitera P, Coates E, Haas NK, Ho K, Khoury R, et al. Detection of primary melanoma in individuals at extreme high risk: a prospective 5-year follow-up study. JAMA Dermatol. 2014;150(8):819-27.
20. Salerni G, Carrera C, Lovatto L, Martí-Laborda RM, Isern G, Palou J, et al. Characterization of 1152 lesions excised over 10 years using total-body photography and digital dermatoscopy in the surveillance of patients at high risk for melanoma. J Am Acad Dermatol. 2012;67(5):836-45.
21. Salerni G, Carrera C, Lovatto L, Puig-Butille JA, Badenas C, Plana E, et al. Benefits of total body photography and digital dermatoscopy ("two-step method of digital follow-up") in the early diagnosis of melanoma in patients at high risk for melanoma. J Am Acad Dermatol. 2012;67(1):17-27.
22. Goodson AG, Florell SR, Hyde M, Bowen GM, Grossman D. Comparative analysis of total body and dermatoscopic photographic monitoring of nevi in similar patient populations at risk for cutaneous melanoma. Dermatol Surg. 2010;36(7):1087-98.
23. Rademaker M, Oakley A. Digital monitoring by whole body photography and sequential digital dermoscopy detects thinner melanomas. J Prim Health Care. 2010;2(4):268-72.
24. Rice ZP, Weiss FJ, DeLong LK, Curiel-Lewandrowski C, Chen SC. Utilization and rationale for the implementation of total body (digital) photography as an adjunct screening measure for melanoma. Melanoma Res. 2010;20(5):417-21.
25. Terushkin V, Oliveria SA, Marghoob AA, Halpern AC. Use of and beliefs about total body photography and dermatoscopy among US dermatology training programs: an update. J Am Acad Dermatol. 2010;62(5):794-803.
26. Nathansohn N, Orenstein A, Trau H, Liran A, Schachter J. Pigmented lesions clinic for early detection of melanoma: preliminary results. Isr Med Assoc J. 2007;9(10):708-12.
27. Risser J, Pressley Z, Veledar E, Washington C, Chen SC. The impact of total body photography on biopsy rate in patients from a pigmented lesion clinic. J Am Acad Dermatol. 2007;57(3):428-34.
28. Banky JP, Kelly JW, English DR, Yeatman JM, Dowling JP. Incidence of new and changed nevi and melanomas detected using baseline images and dermoscopy in patients at high risk for melanoma. Arch Dermatol. 2005;141(8):998-1006.
29. Nehal KS, Oliveria SA, Marghoob AA, Christos PJ, Dusza S, Tromberg JS, et al. Use of and beliefs about baseline photography in the management of patients with pigmented lesions: a survey of dermatology residency programmes in the United States. Melanoma Res. 2002;12(2):161-7.
30. Tiersten AD, Grin CM, Kopf AW, Gottlieb GJ, Bart RS, Rigel DS, et al. Prospective follow-up for malignant melanoma in patients with atypical-mole (dysplastic-nevus) syndrome. J Dermatol Surg Oncol. 1991;17(1):44-8.
31. Slue W, Kopf AW, Rivers JK. Total-body photographs of dysplastic nevi. Arch Dermatol. 1988;124(8):1239-43.
32. Wurm EM, Soyer HP. Scanning for melanoma. Aust Prescr. 2010;33:150-5.
33. Feit NE, Dusza SW, Marghoob AA. Melanomas detected with the aid of total cutaneous photography. Br J Dermatol. 2004;150(4):706-14.
34. Fernandes NC, Calmon R, Maceira JP, Cuzzi T, Silva CSC. Melanoma cutâneo: estudo prospectivo de 65 casos. An Bras Dermatol. 2005;80(1):25-Hornung A, Steeb T, Wessely A, Brinker TJ, Breakell T, Erdmann M, et al. The value of total body photography for the early detection of melanoma: a systematic review. Int J Environ Res Public Health. 2021;18(4):1726.
35. Grupo Brasileiro de Melanoma. Recomendações para o tratamento do melanoma cutâneo. São Paulo: GBM; 2019. Disponível em: https://gbm.org.br/wp-content/uploads/2019/09/Livro-GBM.pdf
36. Kelly JW, Yeatman JM, Regalia C, Mason G, Henham AP. A high incidence of melanoma found in patients with multiple dysplastic naevi by photographic surveillance. Med J Aust. 1997;167(4):191-4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}