


Marco Alexandre Rocha1; Sergio Schalka2; Thais Helena Matsuda Yoshizumi3; Fernanda Calvente Bayan3; Vinicius Fontanesi Blum3
Submitted on: 11/02/2023
Approved on: 10/05/2023
Financial support: The study was funded by the laboratory FARMOQUÍMICA SA, Rio de Janeiro, Brazil.
Conflict of interest: The authors of the study act as speakers for the laboratory that financed the study - FARMOQUÍMICA SA, Rio de Janeiro, Brazil.
Clinical Trial: NCT05216289
Ethics committee number: CAAE: 03728318.5.000
How to cite this article: Rocha MA, Schalka S, Yoshizumi THM, Bayan FC, Blum VF. The efficacy of an oral probiotic associated with a fixed combination of adapalene-benzoyl peroxide in the treatment of acne: a randomized, double-blind, placebo- controlled clinical trial. Surg Cosmet Dermatol. 2023;15:e20230225.
INTRODUCTION: Acne is a chronic inflammatory disease of the pilosebaceous unit of multifactorial origin, which causes a significant impact on quality of life.
OBJECTIVE: Clinical trial assessing the superiority of efficacy of a treatment regimen with an oral probiotic associated with a fixed combination of adapalene 0.1% and benzoyl peroxide 2.5% compared to an oral placebo with the same topical treatment in patients with acne.
METHODS: This was a randomized, double-blind, placebo-controlled study conducted with 212 patients aged from 12 to 35 years. The study was divided into two phases of 90 days each. In the first phase, patients received treatment with adapalene 0.1% and benzoyl peroxide 2.5% associated with a probiotic (IT), or adapalene 0.1% and benzoyl peroxide 2.5% associated with placebo (CT). In the second phase (90 days), patients received only oral treatment with a probiotic or placebo. Efficacy criteria were: reduced Investigator Global Assessment (IGA) scale to 0 or 1 and reduced lesion count.
RESULTS: There was a significant difference in the proportion of participants with IGA 0 or 1 - the arm receiving the test treatment was superior to the control (p<0.05). Both treatments were safe and well tolerated.
CONCLUSION: In light of the evidence on efficacy and safety, treatment with probiotics should be considered as an adjuvant therapy for acne control.
Keywords: Acne vulgaris; Probiotics; Gastrointestinal microbiome
It is estimated that acne affects about 9.4% of the global population, and it is one of the most prevalent diseases worldwide,1 especially in adolescents, affecting 85% of this population.2 The disease impacts significantly the quality of life and is commonly associated with psychiatric disorders such as low self-esteem, social phobias, and depression.3
Acne is a chronic inflammatory disease of the pilosebaceous unit of multifactorial origin, resulting from dysfunction in sebum production, altered infundibular keratinization, inflammation, and bacterial dysbiosis of hair follicles.4
Although the exact way in which these processes interact and the order in which they occur in the pathogenesis of acne is still not fully known,5 recent discoveries about the commensal bacterium Cutibacterium acnes (C. acnes) point to the critical role of the balance between its strains in the pathophysiology of the disease. Contrary to previously thought, the proliferation of C. acnes does not trigger acne, as acne patients do not harbor more strains in their follicles than normal individuals. Instead, loss of skin microbial diversity, with exaggerated activation of innate immunity, may lead to this chronic inflammatory condition.6 The role of C. acnes in the pathophysiology of acne and the inflammatory basis via innate immunity are two factors that have changed treatment approaches. Thus, inflammation became the hallmark of the disease process, from onset to resolution.7
In addition to androgen hormones, recent research has linked insulin and insulin-like growth factor-1 (IGF-1) to the pathophysiological process of acne.8 IGF-1 is related to increased lipogenesis in the sebaceous gland, regardless of androgens,9 and also to the release of inflammatory cytokines. It is noted that serum levels of IGF-1 are higher in adults with acne and correlate quantitatively with the severity of the disease.10 Insulin and IGF-1 activate rapamycin complex 1 (mTORC1) signaling, the regulator key components of anabolism and lipogenesis, while suppressing the metabolic transcription factor FoxO1 activity. FoxO1 is a negative co-regulator of several transcription factors crucial to sebaceous lipogenesis.11
Current acne treatments have several limitations, and increasing antibiotic resistance has diminished their effectiveness.12 Therefore, new effective long-term therapies are needed. Given recent discoveries about the pathophysiology of acne, the loss of diversity of C. acnes strains in the skin and the IGF-1 signaling pathway are important targets for new therapies.13 Considering the effects of probiotics in maintaining intestinal and skin microbiome homeostasis, the effectiveness of using these commensal microorganisms has been investigated in recent clinical studies in acne treatment.12,14,15
Inhibitory effects of probiotics on C. acnes, mediated by antibacterial proteins and bacteriocin-like inhibitory substances, have been demonstrated, in addition to immunomodulatory effects on keratinocytes and epithelial cells.12 Furthermore, treatment with probiotics improved the clinical parameters of patients with acne and also reduced significantly IGF-1 expression and increased FOX01 expression, with statistical significance, in a randomized, placebo-controlled study.15
The effectiveness of probiotics has also been proven as an adjunct therapy to antibiotic acne treatment. A randomized clinical trial with three arms, comparing the use of systemic minocycline to probiotic alone and the combination of both, showed that the group that received the combined treatment with antibiotic and probiotic showed statistically significant results in the total reduction of lesions compared to the other groups. Also, there was a reduction in adverse events resulting from the chronic use of antibiotics. These results suggest that probiotics can be considered a therapeutic option or adjuvant for acne, providing a synergistic anti-inflammatory effect with systemic antibiotics.14
Given the potential outcomes of probiotics in maintaining the balance of the skin microbiota, as well as in insulin/IGF-1 and FOX01 signaling, with consequent positive effects in the treatment of acne, especially when used as adjuvant therapy,14,15 this clinical trial aims to evaluate the comparative efficacy of a regimen containing an oral probiotic (Lactobacillus acidophilus + Bifidobacterium lactis) and topical treatment with adapalene 0.1% and benzoyl peroxide 2.5% in patients with mild to moderate acne.
We recruited 400 participants aged between 12 and 35 years, of both sexes, diagnosed with acne grades II and III, with mixed or oily skin, and skin phototype between I and IV, according to the Fitzpatrick scale. We excluded pregnant, lactating, or intending to become pregnant during the study period patients, as well as individuals who received treatments with corticosteroids and antimicrobials 30 days before selection and those who received immunosuppressant 90 days before selection.
The study was conducted in Osasco (SP), Brazil, at Medcin Instituto da Pele Ltda. , and the study period was from April 18, 2018, to April 7, 2021. The Research Ethics Committee from São Francisco University (SP) approved the study protocol on December 14, 2018. CAAE: 03728318.5.0000.5514. Opinion number: 3,083,043. All participants signed the Informed Consent Form (ICF), and the research was conducted by Good Clinical Practices and the 1996 Declaration of Helsinki. We recruited 400 participants aged between 12 and 35 years, of both sexes, diagnosed with acne grades II and III, with mixed or oily skin, and skin phototype between I and IV, according to the Fitzpatrick scale. We excluded pregnant, lactating, or intending to become pregnant during the study period patients, as well as individuals who received treatments with corticosteroids and antimicrobials 30 days before selection and those who received immunosuppressant 90 days before selection.
The study was conducted in Osasco (SP), Brazil, at Medcin Instituto da Pele Ltda. , and the study period was from April 18, 2018, to April 7, 2021. The Research Ethics Committee from São Francisco University (SP) approved the study protocol on December 14, 2018. CAAE: 03728318.5.0000.5514. Opinion number: 3,083,043. All participants signed the Informed Consent Form (ICF), and the research was conducted by Good Clinical Practices and the 1996 Declaration of Helsinki.
It was a randomized, double-blind, two-arm, placebo-controlled trial. It aimed to assess the superiority of treatment with an oral probiotic composed of Lactobacillus acidophilus, Bifidobacterium lactis, vitamins and minerals - Exímia Probiac® (EP) - combined with the association of topical adapalene 0.1% and benzoyl peroxide 2.5% - Epiduo® (PBA) - compared to the use of PBA associated with placebo in improving the clinical condition of patients with acne.
Eligible participants were randomized into two equal groups to receive one of the treatments. Topical and oral treatments were administered once daily. Patients were also instructed to use SPF 50 sunscreen daily. Everyone received a bottle on the first visit. The company FARMOQUÍMICA SA provided all study samples.
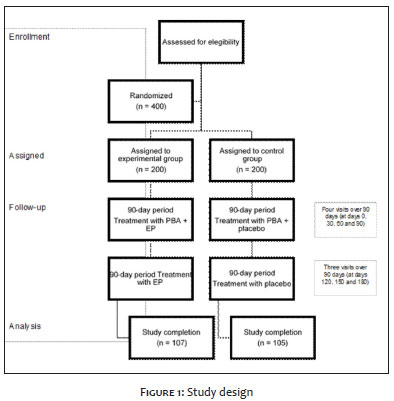
The study was divided into two phases of 90 days each, totaling 180 days. We assessed patients at the initial visit (D0) and then every 30 days, totaling seven visits. On visit D0, patients received randomized treatments and directions for use. In the first phase (90 days), patients received treatment with PBA associated with PE (investigational treatment - IT) or PE associated with placebo (comparator treatment - CT). In the second phase (90 days), patients received only oral treatment with EP or placebo. Figure 1 describes the study design.
At each visit (D0, D30, D60, D90, D120, D150, and D180), we clinically evaluated the patients and recorded the results against the Investigator Global Assessment (IGA) scale.
The primary variables of the study were the reduction of the IGA score to grade 1 or 0, as well as the reduction in the total number of inflammatory and non-inflammatory lesions in the facial region. We considered evaluations according to an established scoring scale to quantify IGA:
0 = Clean skin: residual hyperpigmentation and erythema may be present;
1 = Almost clear: some scattered comedones and a few small papules;
2 = Mild: less than half of the face affected, some comedones and some papules and pustules;
3 = Moderate: more than half of the face affected, some comedones, papules, and pustules. A nodule may be present;
4 = Severe: The entire face is severely affected by comedones, numerous papules and pustules, and some nodules and cysts.
We compared the results obtained from clinical, instrumental, and subjective evaluations between experimental times and, subsequently, between treatments. The hypothesis tests used in the study had a significance level of 95%, and the statistical power of these tests was above 80%. We conducted descriptive analyses of the variables studied using frequency tables and descriptive statistics. The percentage of participants with a reduction in the total number of inflammatory and non-inflammatory lesions and with regression of the IGA scale to no lesions (score 0) or almost no lesions (score 1) were evaluated using the z-test for comparison of two proportions.
Results were considered statistically significant at a significance level of 5% (p≤0.05). The significance level was controlled by rejecting the null hypotheses if the p-value was less than or equal to 5%.
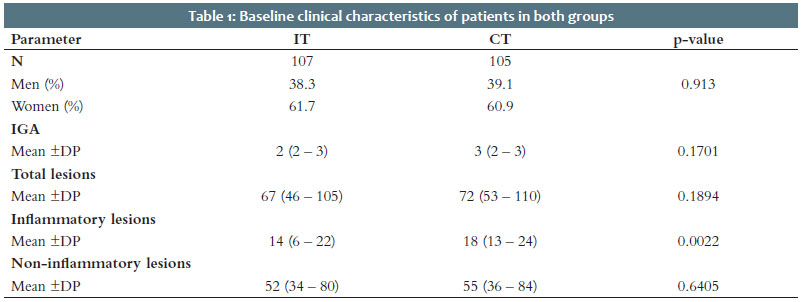
We selected 400 patients. A total of 146 participants were considered lost to follow-up; 34 were excluded due to low adherence; and eight were discontinued due to adverse events. Thus, 212 patients completed the study, 107 in the test treatment group and 105 in the comparator treatment group. The age range of final participants ranged from 12 to 35 years old, with an average of 17 years old. Table 1 describes baseline clinical characteristics. The distribution of patients was homogeneous in both groups.
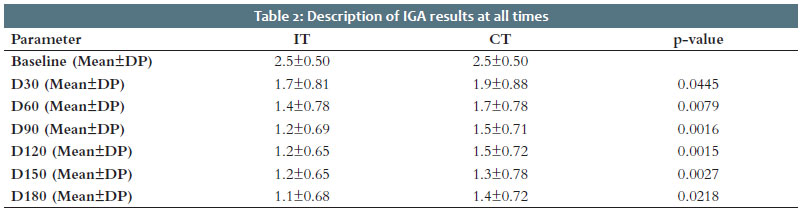
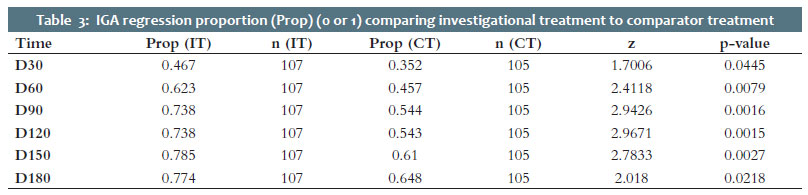
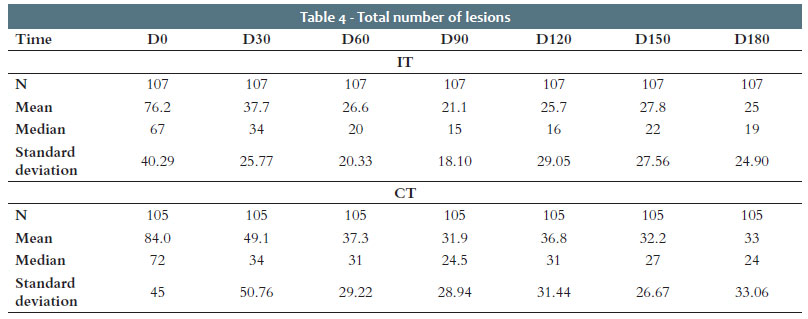
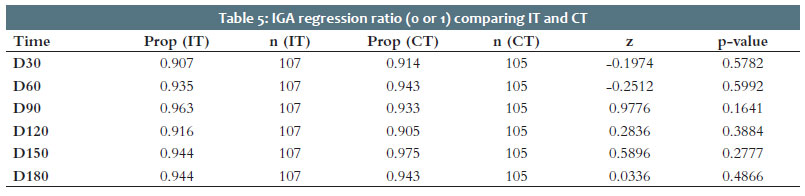
We assessed the primary efficacy parameter, reduction of the IGA scale to 0 or 1, by comparing the proportions at each of the times, starting from D30. Table 2 shows the descriptive results of means and standard deviations of IGA in both groups. We analyzed the proportion of patients with IGA 1 or 0, concerning the total number of patients at that time point ( Table 3), to compare the proportions at each time point from D30 onwards. The results indicate that there was a significant difference in the proportion of participants with IGA 0 or 1, with the IT group being superior to the CT group at all experimental times (p<0.05) (Tables 4 and 5).
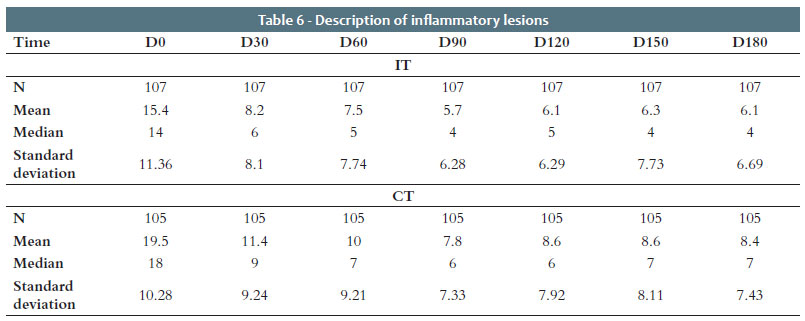
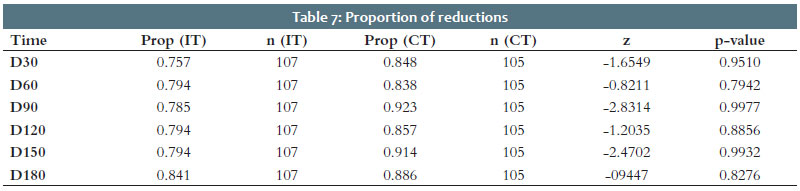
Table 6 depicts descriptive results regarding the number of inflammatory lesions for both groups. Table 7 shows the proportion of patients who showed a reduced count of inflammatory lesions between the determined time and time 0. There was no statistically significant difference (p<0.05) between the two groups at any experimental time. However, at all experimental times, the proportion of patients who showed a reduction in inflammatory lesions was higher in the IT group compared to the CT group, although without statistical significance.
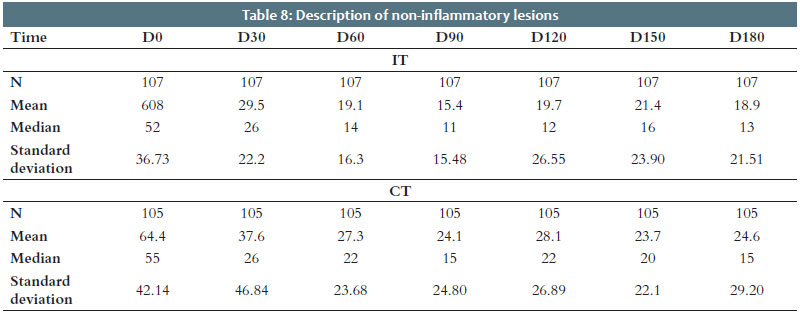
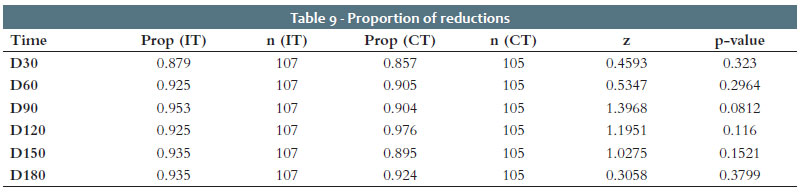
Table 8 depicts descriptive results regarding the number of non-inflammatory lesions for both groups. Table 9 shows the proportion of patients who showed a reduction in the count of non-inflammatory lesions between the determined time and time zero. There was no statistically significant difference (p<0.05) between the two groups at any experimental time. However, at all experimental times, the proportion of volunteers who showed a reduction in inflammatory lesions was higher in the investigational group compared to the comparator group. Nevertheless, without statistical significance.
In the group that received the investigational treatment, one patient had an adverse event that was possibly related, and seven patients had an adverse event that was unlikely to be related to the probiotic drug EP. These events were mild gastrointestinal symptoms such as nausea, stomach pain, and heartburn. In this same group, 73 patients had adverse events related to the topical PBA medication. Of these, one was categorized as product-related, 37 as probable, 30 as possible, and five as unlikely. These events were skin signs and symptoms, such as erythema, edema, itching, and burning at the application site. All patients recovered or remained stable.
The group that received the control treatment reported one adverse event possibly related and one adverse event unlikely related to the placebo treatment. In this group, 70 patients had adverse events related to the use of PBA. These events were skin signs and symptoms, such as erythema, edema, itching, and burning at the application site. Of these, 33 were categorized as probable, 29 as possible, and eight as unlikely concerning the investigational product. All patients recovered.
The data obtained in the present study demonstrate that the use of oral probiotics (Lactobacillus acidophilus and Bifidobacterium lactis) associated with the fixed combination of adapalene 0.1% and benzoyl peroxide 2.5% presents superior efficacy than the same topical product associated with placebo to treat mild to moderate acne. One of the primary efficacy parameters of the study was the reduction of the IGA scale score to 0 or 1. The scale in question has five categories, from 0 to 4, where 0 means total absence of lesions and 4 indicates the greatest severity of acne, with the patient's entire face severely affected by comedones, papules, pustules, and some nodules and cysts. At the first study visit, the mean IGA in both groups (IT and CT) was 2.5, with a standard deviation of 0.5. The first phase of the study lasted 90 days, with visits every 30 days. In all these visits, there was a superiority in the proportion of patients with IGA 0 or 1 in the group that received the investigational treatment concerning the comparator group (p<0.05). At the 90-day visit, the mean IGA in the group that received the investigational treatment was 1.2, with a standard deviation of 0.69. In the comparator group, the mean IGA was 1.5, with a standard deviation of 0.71 (p<0.05).
In the second phase of the study, which lasted 90 days, we suspended the topical treatment so that the test group continued to receive oral treatment with probiotics and the control group continued to receive a placebo. During this period, the IGA averages were lower in all evaluations (120, 150, and 180 days) for the group that received probiotic treatment, and, in the last visit, the value found for this group was 1.1, with a standard deviation of 0.68, compared to 1.4 in the control group, with a Standard deviation of 0.72 (p<0.05).
The data also revealed a tendency towards superior results in the group that received the investigational treatment concerning the reduction in the total number of lesions, inflammatory and non-inflammatory lesions, although without statistical significance.
The administration of EP treatment for 90 days proved to be safe in the studied population, with only one patient having an adverse event possibly related to the therapy and seven patients having adverse events that were unlikely related to the treatment. These events were mild gastrointestinal symptoms, such as nausea, stomach pain, and heartburn, and did not determine the discontinuation of patients from the study.
The set of data presented indicates that, under the circumstances and limitations defined in the present study, treatment with the probiotic EP associated with the topical medication, composed of adapalene 0.1% and benzoyl peroxide 2.5%, is more effective than that treatment consisting of adapalene 0.1% and benzoyl peroxide 2.5% alone in patients with mild to moderate acne, with few reported adverse events.
A recent article by Navarro-López et al. (2021)16 reported a growing number of current studies relating intestinal and cutaneous dysbiosis with the pathophysiology of acne, as well as with other diseases, such as atopic dermatitis and psoriasis. Several studies provide evidence of the influence of probiotic treatments aimed at modulating the skin and intestinal microbiota in these diseases and the positive impact of orally administered probiotics on these dermatoses. Although clinical studies with probiotics to treat acne are still scarce in the literature, several current studies have demonstrated a decrease in the intestinal microbiota diversity in patients with acne.17,18 Therefore, it is plausible to think that probiotics as adjuvant therapy have a relevant role in the treatment and prognosis of this disease.
In 2013, Jung et al. used a probiotic mixture with strains of Lactobacillus acidophilus, Lactobacillus delbrueckii bulgaricus, and Bifidobacterium bifidum in 45 adults with acne. There was a 67% reduction in lesion counts at 12 weeks of treatment and an 82% reduction when the probiotic mixture was combined with oral minocycline.14 These data are consistent with those found in this study, although there was no oral antibiotic treatment. If we consider the 90-day visit our study had a 72% reduction in the number of lesions in the group that received investigational treatment.
In a 2021 clinical study, Kim et al. demonstrated a 33.2% decrease in the total lesion count after 12 weeks of treatment with Lactobacillus bulgaricus and Streptococcus thermophiles.19 Fabbrocini et al. found similar results in a study analyzing the effect of administering Lactobacillus rhamnosus to a group of 20 individuals with acne for 12 weeks, obtaining a 32% reduction (p<0.001) on a 5-point scale.
Although these studies used only probiotics in the evaluation, the results corroborate those found in this study. While the comparison between groups was not statistically significant in terms of lesion count, there was a significant reduction in the number of lesions. At the first visit, the average number of total lesions in the IT group was 76.2, with a standard deviation of 40.29, and, at the 180-day visit, this average was reduced to 25, with a standard deviation of 24.9.
Currently, there is a need for alternatives to the use of oral antibiotics for the treatment of acne. We know that these medications are associated with risks, especially when taken for a long time, such as opportunistic infections, gastrointestinal inflammatory processes, and the development of bacterial resistance.20 Their prescription is justified by their anti-inflammatory action and not by their antibacterial activity.21 Therefore, oral probiotics, due to their immunomodulatory properties and lower potential to cause side effects, find a real possibility, when associated with other classic alternatives, to enhance the treatment of acne.
It is the first clinical trial to compare the use of oral probiotics associated with topical treatment in Brazilian patients. In this clinical trial, the treatment period was 180 days, a relatively long period compared to several similar clinical trials. The sample size was sufficient for the robustness of the data found. The study methodology, as well as the efficacy parameters such as the IGA scale and the reduction in the number of lesions, provided an absolute quantitative measure of improvement, and other clinical trials have used these same endpoints.22 Blinding of the raters that generate these results for treatment allocations also allowed us to avoid the evaluation bias. New studies need to quantitatively and qualitatively assess the skin and gut microbiome before and after treatment, as well as the primary mediators and proteins involved, such as substance P, IGF-1 expression, insulin, and interleukin,17 among others.
Exímia Probiac® associated with the Epiduo® product showed superior efficacy than treatment with Epiduo® associated with placebo in reducing the IGA scale in patients with mild to moderate acne, with statistical significance, and in reducing the number of lesions (inflammatory and non-inflammatory), without statistical significance. The test treatment was safe and well tolerated. The evidence on efficacy and safety shows that Exímia Probiac® should be considered in adjuvant therapy for acne control.
Observation: this was a sponsored study.
Marco Alexandre Rocha
ORCID: 0000-0003-1090-177X
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Sergio Schalka
ORCID: 0000-0003-2425-7962
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
Thais Helena Matsuda Yoshizumi
ORCID: 0000-0002-7197-5118
Approval of the final version of the manuscript effective participation in research orientation; critical review of the manuscript.
Fernanda Calvente Bayan
ORCID: 0000-0002-2455-939X
Approval of the final version of the manuscript; critical review of the manuscript.
Vinicius Fontanesi Blum
ORCID: 0000-0002-3202-2453
Approval of the final version of the manuscript; critical review of the manuscript.
1. Tan JK, Bhate K. A global perspective on the epidemiology of acne. Br J Dermatol. 2015;172(Suppl 1):3-12.
2. Habeshian KA, Cohen BA. Current issues in the treatment of acne vulgaris. Pediatrics. 2020;145(Suppl 2):S225-S30.
3. Koo JY, Smith LL. Psychologic aspects of acne. Pediatr Dermatol. 1991;8(3):185-8.
4. Williams HC, Dellavalle RP, Garner S. Acne vulgaris. Lancet. 2012;379(9813):361-72.
5. Cooper AJ, Harris VR. Modern management of acne. Med J Aust. 2017;206(1):41-5.
6. Dréno B, Pécastaings S, Corvec S, Veraldi S, Khammari A, Roques C. Cutibacterium acnes (Propionibacterium acnes) and acne vulgaris: a brief look at the latest updates. J Eur Acad Dermatol Venereol. 2018;32(Suppl 2):5-14.
7. Kircik LH. Re-evaluating treatment targets in acne vulgaris: adapting to a new understanding of pathophysiology. J Drugs Dermatol. 2014;13(6):s57-60.
8. Cong TX, Hao D, Wen X, Li XH, He G, Jiang X. From pathogenesis of acne vulgaris to anti-acne agents. Arch Dermatol Res. 2019;311(5):337-49.
9. Ozdarska K, Osucha K, Savitskyi S, Malejczyk J, Galus R. Rola diety w patogenezie trądzika pospolitego [Diet in pathogenesis of acne vulgaris]. Pol Merkur Lekarski. 2017;43(256):186-9.
10. Osher E, Macaulay VM. Therapeutic targeting of the IGF axis. Cells. 2019;8(8):895.
11. Aktaş Karabay E, Saltık ZA, Unay Demirel Ö. Evaluation of serum FoxO1, mTORC1, IGF-1, IGFBP-3 levels, and metabolic syndrome components in patients with acne vulgaris: a prospective case-control study. Dermatol Ther. 2020;33(6):e13887.
12. Goodarzi A, Mozafarpoor S, Bodaghabadi M, Mohamadi M. The potential of probiotics for treating acne vulgaris: a review of literature on acne and microbiota. Dermatol Ther. 2020;33(3):e13279.
13. Dessinioti C, Dreno B. Acne treatments: future trajectories. Clin Exp Dermatol. 2020;45(8):955-61.
14. Jung GW, Tse JE, Guiha I, Rao J. Prospective, randomized, open-label trial comparing the safety, efficacy, and tolerability of an acne treatment regimen with and without a probiotic supplement and minocycline in subjects with mild to moderate acne. J Cutan Med Surg. 2013;17(2):114-22.
15. Fabbrocini G, Bertona M, Picazo Ó, Pareja-Galeano H, Monfrecola G, Emanuele E. Supplementation with Lactobacillus rhamnosus SP1 normalises skin expression of genes implicated in insulin signalling and improves adult acne. Benef Microbes. 2016;7(5):625-30.
16. Navarro-López V, Núñez-Delegido E, Ruzafa-Costas B, Sánchez-Pellicer P, Agüera-Santos J, Navarro-Moratalla L. Probiotics in the therapeutic arsenal of dermatologists. Microorganisms. 2021;9(7):1513.
17. Deng Y, Wang H, Zhou J, Mou Y, Wang G, Xiong X. Patients with acne vulgaris have a distinct gut microbiota in comparison with healthy controls. Acta Derm Venereol. 2018;98(8):783-90.
18. Yan HM, Zhao HJ, Guo DY, Zhu PQ, Zhang CL, Jiang W. Gut microbiota alterations in moderate to severe acne vulgaris patients. J Dermatol. 2018;45(10):1166-71.
19. Kim MJ, Kim KP, Choi E, Yim JH, Choi C, Yun HS, et al. Effects of Lactobacillus plantarum CJLP55 on clinical improvement, skin condition and urine bacterial extracellular vesicles in patients with acne vulgaris: a randomized, double-blind, placebo-controlled study. Nutrients. 2021;13(4):1368.
20. Thiboutot DM, Dréno B, Abanmi A, Alexis AF, Araviiskaia E, Barona Cabal MI, et al. Practical management of acne for clinicians: an international consensus from the global alliance to improve outcomes in acne. J Am Acad Dermatol. 2018;78(2 Suppl 1):S1-S23.
21. Leyden JJ, Del Rosso JQ, Webster GF. Clinical considerations in the treatment of acne vulgaris and other inflammatory skin disorders: focus on antibiotic resistance. Cutis. 2007;79(6 Suppl):9-25.
22. Semprini A, Braithwaite I, Corin A, Sheahan D, Tofield C, Helm C, et al. Randomised controlled trial of topical kanuka honey for the treatment of acne. BMJ Open. 2016;6(2):e009448.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}