


Gabrieli Budke Tiecher1; João Victor Bezerra1; Beatriz Freitas Filitto1; Marilda Aparecida Milanez Morgado de Abreu1; Hélio Amante Miot2; Ana Claudia Cavalcante Espósito1,2
Submitted on: 02/04/2023
Approved on: 28/08/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Tiecher GB, Bezerra JV, Filitto BF, Abreu MAMM, Miot HA, Espósito ACC. Keratoacanthoma centrifugum marginatum: report of a rare variant of keratoacanthoma. Surg Cosmet Dermatol. 2023;15:e20230244.
We report a case of a 72-year-old man who underwent surgical excision of a keratoacanthoma centrifugum marginatum (KCM) located on the left forearm. It is an uncommon variant of keratoacanthoma, which can assume large dimensions (up to 20 cm) and does not tend to spontaneous regression. The lesion is usually single, with raised borders, and has progressive centrifugal growth associated with central healing and atrophy. Due to its rarity and lack of pathognomonic histopathological features, KCM can be a diagnostic challenge for dermatologists and pathologists.
Keywords: Keratoacanthoma; Neoplasms; Skin neoplasms
Keratoacanthoma centrifugum marginatum (KCM) is a rare variant of keratoacanthoma, first described by Miedzinski and Kozakiewicz in 1962.1 Typically, the lesion is a single plaque with raised edges, with peripheral centrifugal growth, associated with simultaneous central scarring.2
KCM is composed of keratinizing squamous cells originating from pilosebaceous follicles.1,3 It grows rapidly and, unlike classic keratoacanthoma, does not tend to spontaneous regression, in addition to being able to assume large dimensions (up to 20cm).3,4 Although locally destructive, KCM is a tumor with a low risk of metastasis, as are other keratoacanthoma lesions.5
A 72-year-old man, a smoker, without other comorbidities or use of medication, sought care due to the appearance, three months ago, of a lesion on the posterior surface of his right forearm, which was rapidly growing and painless. The patient denied a family history of similar injuries or local trauma. He denied occupational exposure to chemicals or prior treatment for the lesion. He reported intense photoexposure during adulthood without photoprotection measures.
Dermatological examination showed an erythematous plaque, not infiltrated on palpation, with an ulcerated and atrophic center, measuring 7 x 4 cm, with raised, well-defined, discretely hyperkeratotic edges (Figure 1A) on the posterior surface of the right forearm. There was no axillary lymph node enlargement on palpation.
The patient underwent surgical excision of the lesion with a safety margin (1 cm). The resulting surgical defect was closed through total skin grafting, using triangular redundancy of adjacent skin (“dog ear”) – local graft (Figure 1B).
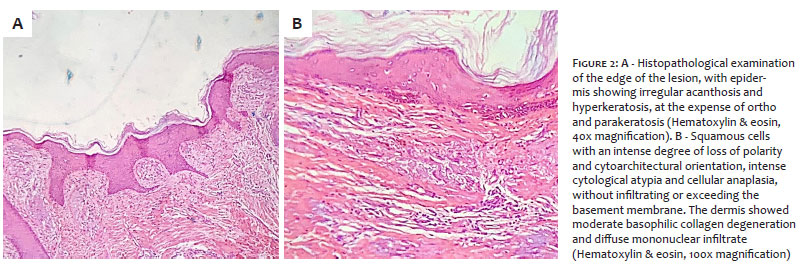
The histopathological examination showed an epidermis with irregular acanthosis and hyperkeratosis at the expense of ortho and parakeratosis. The squamous cells exhibited intense loss of polarity and cytoarchitectural orientation, with severe cytological atypia and cellular anaplasia, without infiltrating or surpassing the basement membrane. The dermis showed moderate basophilic collagen degeneration and diffuse mononuclear infiltrate. Given the clinical and histopathological findings, the definitive diagnosis was keratoacanthoma centrifugum marginatum with free resection margins (Figures 2A and B).
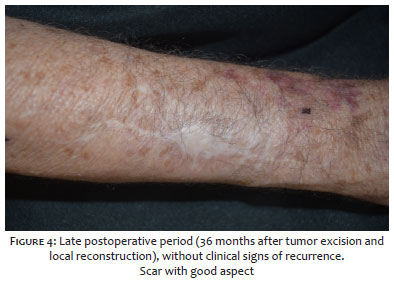
On the 21st postoperative day, the patient presented deepithelialization in the central portion of the graft (Figure 3), but it progressed to spontaneous healing after two weeks. The patient continues to be under clinical follow-up at the institution’s Dermatology Service for 36 months without recurrence (Figure 4).
Keratoacanthomas are fast-growing tumors composed of keratinocytes originating from the follicular infundibulum epithelium.5 KCM is a rare variant of keratoacanthoma, whose main characteristics are generally a single lesion, which can be large (up to 20 cm), with raised edges, and progressive centrifugal growth associated with central healing and atrophy. Unlike classic keratoacanthoma, it does not tend to regress spontaneously.3,5 Its incidence is not known.6
The sites most frequently affected by KCM are the head and neck, and the upper and lower limbs of adults.4 The risk factors for its development are the same as those that lead to the emergence of classic keratoacanthomas or squamous cell carcinomas: exposure to ultraviolet radiation, smoking, and exposure to other chemical carcinogens.3 There are five reports of cases of KCM that developed in a trauma area.7 The literature brings together around seven cases of individuals with multiple KCM injuries; all others are reports of isolated injuries.8 Although uncommon in this age group, there is a report of a five-year-old boy with multiple KCM injuries in the lower limbs.8
The main diagnostic differentials are fungal infection, atypical mycobacteriosis, botryomycosis, pyoderma gangrenosum, squamous cell carcinoma, and cutaneous lupus erythematosus.4 The definitive diagnosis of KCM can be a challenge for the dermatologist, requiring a high level of clinical suspicion. An incisional biopsy may not be able to define the diagnosis, requiring serial biopsies or a definitive diagnosis after analysis of the complete surgical specimen.9,10
Histologically, the KCM margin tends to present the classic findings of keratoacanthoma, while the central portion has atrophic or healing tissue.6 There is a central crater filled with keratin, with prominent edges and a clear delineation between the tumor nests and the stroma, in addition to the absence of stromal anaplasia and desmoplasia.11
The gold standard in the KCM treatment is surgical excision, generally by conventional surgery. Micrographic surgery tends to be restricted to cases of recurrent KCM, in lesions with poorly defined borders, of extremely rapid growth, or when preserving healthy skin is mandatory.6 In very large lesions, or when surgical approaches are not possible, oral retinoids, intralesional methotrexate, phototherapy, or bleomycin are therapeutic options.9,12,13
KCM is a rare variant of keratoacanthoma, and its diagnosis can be a challenge for the attending physician due to the absence of pathognomonic histopathological characteristics. Usually, it is a single, large lesion (up to 20 cm) with raised edges and progressive centrifugal growth associated with central healing and atrophy. It does not tend to regress spontaneously, and surgical excision is the therapy of choice whenever possible, given the size and location of the lesion.
Gabrieli Budke Tiecher
ORCID: 09-0004-5338-5036
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical review of the manuscript.
João Victor Bezerra
ORCID: 00-0002-7938-8794
Approval of the final version of the manuscript; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
Beatriz Freitas Filitto
ORCID: 00-0002-0196-814X
Approval of the final version of the manuscript; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Marilda Aparecida Milanez Morgado de Abreu
ORCID: 00-0001-9099-6013
Approval of the final version of the manuscript; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Hélio Amante Miot 0000-0002-2596-9294
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; effective participation in research orientation; critical literature review; critical review of the manuscript.
Ana Claudia Cavalcante Espósito
ORCID: 00-0001-9283-2354
Approval of the final version of the manuscript; conception and planning of the study; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; effective participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
1. Miedzinski F, Kozakiewicz J. Keratoacanthoma centrifugum - a special variety of keratoacanthoma. Hautarzt Z Dermatol Venerol Verwandte Geb. 1962;13:348–52.
2. Kwiek B, Schwartz RA. Keratoacanthoma (KA): an update and review. J Am Acad Dermatol. 2016;74(6):1220–33.
3. Divers AK, Correale D, Lee JB. Keratoacanthoma centrifugum marginatum: a diagnostic and therapeutic challenge. Cutis. 2004;73(4):257–62.
4. Xiao H, Hooper PB, Umphress BA, Wolverton JE. Keratoacanthoma centrifugum marginatum. Dermatol Online J. 2021;27(3):13030/qt5vp5f7bq.
5. Dominiak N, Hayes B, Swick J, Leach B, Maize J, Ralston J. Keratoacanthoma centrifugum marginatum: a diagnostic and therapeutic challenge. JAAD Case Rep. 2016;2(3):206–8.
6. Ratnapala D, Lambrianides A, Mahoney H. Keratoacanthoma centrifugum marginatum. ANZ J Surg. 2006;76(4):277–8.
7. Gavric G, Lekic B, Milinkovic SM, Bosic M, Zivanovic D. Keratoacanthoma centrifugum marginatum associated with mechanical trauma: response to acitretin – a case report and review of the literature. Dermatol Ther. 2020;33(3):e13397.
8. Dogra S, Vinay K, Saikia UN, De D, Handa S. Multiple keratoacanthoma centrifugum marginatum in a young boy, and review of the literature. Clin Exp Dermatol. 2017;42(6):711–3.
9. Ogasawara Y, Kinoshita E, Ishida T, Hamamoto Y, Fujiyama J, Muto M. A case of multiple keratoacanthoma centrifugum marginatum: response to oral etretinate. J Am Acad Dermatol. 2003;48(2):282–5.
10. Silva E, Estébanez A, Martín JM, Monteagudo C, Montesinos E. Keratoacanthoma centrifugum marginatum after photodynamic therapy with good response to oral retinoids and topical 5-fluorouracil. Dermatol Ther. 2019;32(4):e12988.
11. V’lckova-Laskoska MT, Laskoski DS. Keratoacanthoma centrifugum marginatum: a rare atypical variant of keratoacanthoma. Clin Exp Dermatol. 2008;33(3):259–61.
12. De la Torre C, Losada A, Cruces MJ. Keratoacanthoma centrifugum marginatum: treatment with intralesional bleomycin. J Am Acad Dermatol. 1997 Dec;37(6):1010-1.
13. Qi S, Huang T, Zhu D, Pan H, He R. Keratoacanthoma centrifugum marginatum: an unusual case. Photodiagnosis Photodyn Ther. 2021;36:102468.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}