


Khairuddin Djawad; Siswanto Wahab
Submitted on: 31/01/2023
Approved on: 23/02/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Djawad K, Wahab S. Sclerosing lipogranuloma of the penis: reconstruction using double reverse V-Y-plasty. Surg Cosmet Dermatol. 2023;15:e20230222.
Sclerosing lipogranuloma is a chronic granulomatous reaction in response to the injection of non-medical substances such as paraffin, silicone, or mineral oil into the skin. This report describes one case of a large defect on the penis following sclerosing lipogranuloma excision surgery that was successfully closed by a double reverse V- Y-plasty reconstruction. The surgery aimed to remove all affected tissue as soon as possible, preventing the persistent granulomatous process that leads to necrosis and severe penile deformity. The double reverse V- Y-plasty is a simple, single-stage procedure useful to reconstruct of a large defect on the penis.
Keywords: Granuloma; Sclerosing solutions; Surgery.
Sclerosing lipogranuloma, or penile paraffinoma, is a granulomatous foreign body inflammation of the reticular and subcutaneous dermis resulting from subcutaneous injection of non-medical exogenous substances into the penis.1 The injection of non-medical substances into the skin of the penis aimed to increase penis size or treat sexual dysfunction. This practice is influenced by psychological factors such as low self-confidence, unsatisfactory sexual intercourse, and problems of social deviation.2 The prevalence of penile enlargement injections tends to increase in Asian and Eastern European countries.3 Downey, et al. reported 124 cases of paraffinoma from various literatures between 1956–2017 and found that the average age of patients was 36.3 years.4 Treatment modalities for sclerosing lipogranuloma of the penis include a conservative approach, using various dressings, antibiotics, or pain medication, and the definitive treatment is surgical excision to remove the damaged tissue.5 We report a case of a 35- year-old man presenting sclerosing lipogranuloma of the penis, confirmed through history, physical examination, and histopathological examination. The patient underwent radical excision of the granuloma tissue, followed by a double reverse V-Y-plasty reconstruction with excellent results.
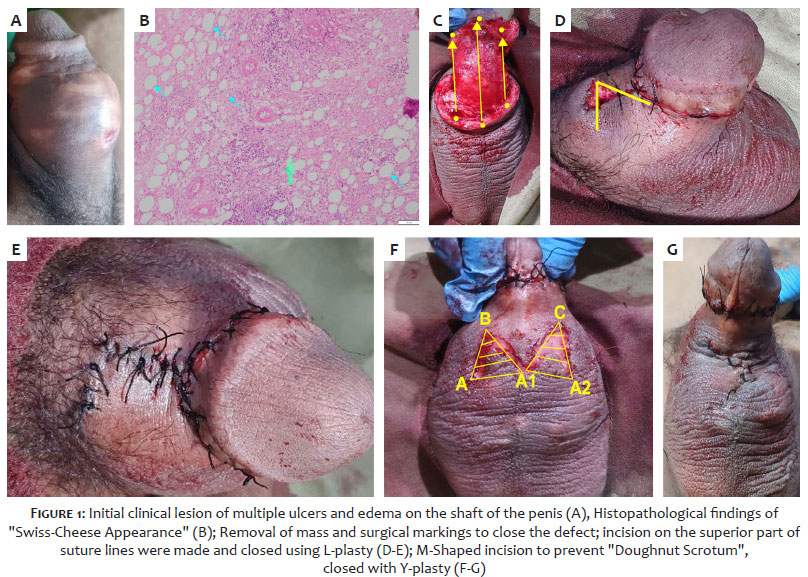
A 35-year-old man visited the outpatient clinic complaining of edema on the shaft of the penis six for months. The complaint was accompanied by severe pain for three months. The patient stated that non-medical personnel had injected candlenut oil twice into the skin of the penis shaft, approximately 10 mL each, three years ago, with an interval of 6 months between injections, as he was not satisfied with his penis size. He denied a history of disorders of urination, erection, and ejaculation. The patient also negated a history of diabetes mellitus and hypertension. Physical examination found his vital signs were within normal limits. Venereological examination of the penile region found multiple ulcers and edema on the shaft of the penis. Upon palpation, a tender, solid, and hard mass with indeterminate boundaries was found. The testis, scrotum, suprapubic, and lymphatic vessels showed no abnormalities (Figure 1A).
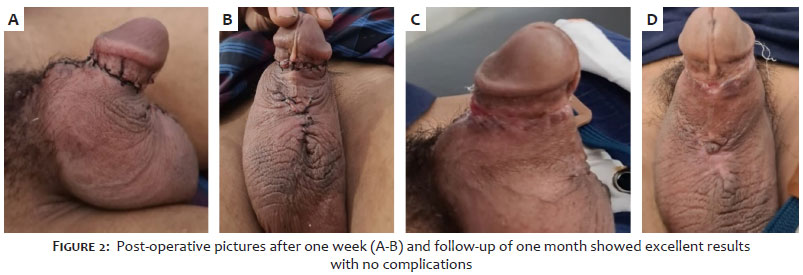
After anamneses and physical examination, histopathological examination confirmed the diagnosis of sclerosing lipogranuloma, showing the typical “Swiss cheese appearance” (Figure 1B). A surgical excision was planned to remove granulomatous tissue from the penile shaft. We started the procedure by making an incision around the shaft of the penis followed by the removal of the mass on the affected tissue. The resulting defect was closed using the scrotal skin as the donor area. (Figure 1C). We assessed the patient for bleeding. A horizontal incision on the superior part of the sutures was made to remove excess skin on the edges and closed using L-plasty (Figures 1D and 1E). The operation continued with the reconstruction to prevent doughnut scrotum and buried penis by an M-shaped incision on the scrotum (Figure 1F), and the wound was closed with a Y-plasty (Figures 1F-G). Post-operative pictures after one week (Figures 2A-B) and follow-up of one month (Figures 2 C-D) showed excellent results with no surgical complications such as tissue necrosis.
Cases of sclerosing lipogranuloma of the penis, as the one reported in this article, tend to increase in recent years. The patient initially complained of chronic pain on the shaft of the penis. These clinical symptoms depend on the amount, substance, location, depth, and duration of the injection.2 Clinical symptoms arise from inflammation of the surrounding injection area, including erythema and edema. Over time, complications can arise with the formation of ulcers or fistula, causing penile deformity, abnormalities in the prepuce (non-reducible paraphimosis and phimosis), Fournier’s gangrene, erectile dysfunction, and voiding dysfunction.6 Another fatal complication is sepsis, and malignancy, as highlighted in one case report of squamous cell carcinoma of the penis after the injection of mineral oil. However, this may take a longer duration: up to 35 years after the initial injection.4
Candlenut oil injected may trigger sclerosing lipogranuloma through several mechanisms. It began with a reaction to a foreign body due to a lack of an enzyme that metabolizes exogenous interstitial oil. This paraffin oil then fills the subcutaneous fat cavity until it is finally surrounded by fibrous tissue, leading to a granulomatous chronic inflammatory reaction.7 Granuloma formation usually occurs within 2–40 days after injection of non-medical substances, followed by complicated lesions.8 This pathogenesis process gives our patient the typical histopathological of Swiss cheese appearance.3
The treatment approach includes resection of the skin with granulomas and ulcers followed by a reconstruction to close the defect. We opted to use the scrotal area as a donor site due to its laxity and because the defect was unamendable using primary sutures and thus might cause retraction. We performed a horizontal incision on the penile shaft above the initial sutures using L-plasty to remove the excess skin, achieve a cosmetic appearance regarding the penile RSTL, prevent suture detachment, and facilitate penile erection. To close the scrotal defect, we chose a double reverse V-Y-plasty technique. We aimed to prevent buried penis and doughnut scrotum and achieve functional and cosmetical outcomes. Scrotal skin was used because of its elastic features.9 The double reverse V-Y-plasty reconstruction technique is derived from the V-Y-plasty technique. An inverted V-shaped incision was made at the midline (raphe) of the scrotum, thus forming an M-shape. We sutured the resulting defect using non-absorbable thread, resulting in a Y-shape. This technique is preferable to the Z incision technique as it produces better aesthetic outcomes and is used widely by plastic surgeons.9-11
Sclerosing lipogranuloma is a complication caused by injecting substances into the penile shaft. Excision followed by removing the substance is the definitive treatment, and the resulting defect can be amended using the double reverse V-Y-plasty technique with excellent results.
Khairuddin Djawad
ORCID: 00-0002-4569-6385
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Effective participation in research orientation; Intellectual participation in propaedeutic and/or therapeutic management of studied cases; Manuscript critical review; Critical literature review.
Siswanto Wahab
ORCID: 00-0002-4895-7683
Approval of the final version of the manuscript; Manuscript critical review.
1. Foxton G, Vinciullo C, Tait CP, Sinniah R. Sclerosing lipogranuloma of the penis. Australas J Dermatol. 2011;52(3):e12-4.
2. Soebhali B. Penile self-injections for girth augmentation: treatment of complications. Textbook of Male Genitourethral Reconstruction: Springer; 2020:783-94.
3. Ahmed U, Freeman A, Kirkham A, Ralph DJ, Minhas S, Muneer A. Self injection of foreign materials into the penis. Ann R Coll Surg Engl. 2017;99(2):e78-e82.
4. Downey AP, Osman NI, Mangera A, Inman RD, Reid SV, Chapple CR. Penile paraffinoma. Eur Urol Focus. 2019;5(5):894-8.
5. Svensøy JN, Travers V, Osther PJS. Complications of penile self-injections: investigation of 680 patients with complications following penile self-injections with mineral oil. World J Urol. 2018;36(1):135-43.
6. De Siati M, Selvaggio O, Di Fino G, Liuzzi G, Massenio P, Sanguedolce F, et al. An unusual delayed complication of paraffin self-injection for penile girth augmentation. BMC Urol. 2013;13:66.
7. Dellis AE, Nastos K, Mastorakos D, Dellaportas D, Papatsoris A, Arkoumanis PT. Minimal surgical management of penile paraffinoma after subcutaneous penile paraffin injection. Arab J Urol. 2017;15(4):387-90.
8. Francis J, Poh Choo Choo A, Wansaicheong Khin-Lin G. Ultrasound and MRI features of penile augmentation by "Jamaica Oil" injection. A case series. Med Ultrason. 2014;16(4):372-6.
9. Mylarappa P, Puvvada S, Nayak K A. Evaluation and outcome of M plasty for the management of doughnut scrotum. J Clin Urol. 2017;10(4):364-7.
10. Manjunath K, Venkatesh M. M-plasty for correction of incomplete penoscrotal transposition. World J Plast Surg. 2014;3(2):138-41.
11. Ammirati CT, Sengelmann RD. Advancement flaps. In: Rohrer TE, Cook JL, Nguyen TH, Mellette JR Jr. Flaps and grafts in dermatologic surgery. Philadelphia: Elsevier; 2007. p. 41-58.
ETHICAL CLEARANCE: The authors have gained informed consent from the patient for his pictures to be documented and published
ACKNOWLEDGEMENTS: The authors thank Jonathan Kurnia Wijaya, MD, Pg.Dip(Derm) and Novita MD for the design and editing of the manuscript.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}