


Liza Castro Rego; Nathalia Calado Melges; José Matheus Frizzo Lopes Moço; Thais Teixeira Libonati; José Antonio Jabur da Cunha
Submitted on: 31/01/2023
Approved on: 23/02/2023
Financial support: None.
Conflict of interest: None.
How to cite this article: Rego LC, Melges NC, Moço JMFL, Libonati TT, Cunha JAJ. Combining two easy performance techniques for the reconstruction of lower lip defects: myomucosal advance flap and M-plasty. Surg Cosmet Dermatol. 2023;15:e20230219.
Small surgical defects of the lower lip can be reconstructed through direct closure. Full-thickness defects with more than 30% involvement require complex reconstructions with high morbidity. We report the case of a patient diagnosed with squamous cell carcinoma in the lower lip whose resection resulted in a surgical defect of 45% of the lower lip. The reconstruction combined two well-established techniques: unilateral myomucosal advancement flap and M-plasty. This association acted synergistically, enabling the closure of the surgical defect with easy execution, low morbidity, and excellent aesthetic and functional results.
Keywords:
Small surgical defects of the lower lip can be reconstructed through direct closure. Full-thickness defects with more than 30% involvement require complex reconstructions with high morbidity. We report the case of a patient diagnosed with squamous cell
Malignant lip tumors occur most frequently in the lower lip, and approximately 2/3 are squamous cell carcinomas (SCC). They are more frequent in the fifth, sixth, and seventh decades of life, prevailing in whites and men in a ratio of 5:1. Chronic exposure to the sun, smoking, and alcoholism are the main risk factors associated with this neoplasm.1
Lip SCCs have a good prognosis when diagnosed early, with a cure rate of around 90% in five years. Surgical removal is the treatment of choice; however, metastases may occur in cervical lymph nodes in 5% to 20% of cases.2
The choice of the technique used for lip reconstruction after surgical removal must be adequate and individualized for each type of defect, considering the location, size, skin elasticity, and the patient’s general condition.1
In the case of surgical defects located in the lower lip, reconstruction techniques are usually categorized according to the percentage of site involvement, and they are divided into small (≤30%), medium (30% to 70%), or large (≥70%) defects.3 Small surgical defects of the lower lip can be reconstructed using direct closure. On the other hand, full-thickness defects with more than 30% involvement require complex reconstructions with high morbidity.
Given the complexity of the numerous procedures, we report a combination of two well-established, easy-to-perform techniques, which were adequate to reconstruct a surgical defect in the lower lip with involvement of 45% of the extension.
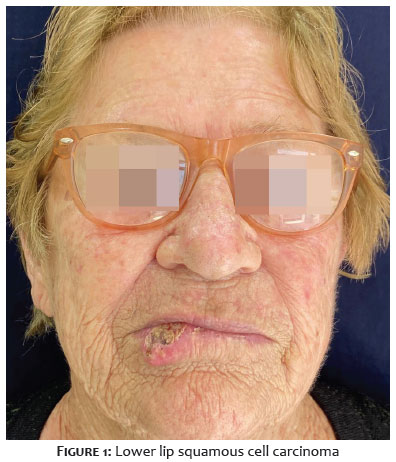
An 81-year-old woman, Fitzpatrick skin phototype II, rural worker, presented to the Dermatology Service with a progressively growing tumor lesion affecting the lower lip for six months. She had a personal history of hypertension and was in the use of atenolol and hydrochlorothiazide. Also, she was an ex-smoker with a smoking load of 65 packs/year. The dermatological examination revealed an ulcerated tumor measuring 40 x 30 mm without involvement of the labial commissures (Figure 1).
Physical examination identified no lymphadenopathy in the cervical and parotid chains. The anatomopathological assessment of the incisional biopsy showed well-differentiated SCC. The patient was referred for surgical treatment.
The procedure was performed under local anesthesia. Initially, two hemostatic stitches using 2-0 nylon thread were placed on the lower lip adjacent to each labial commissure, aiming to compress the inferior labial artery.
We removed the tumor, resulting in a full-thickness surgical defect corresponding to 45% of the length of the lower lip (Figure 2). We opted for reconstruction with a unilateral myomucosal advancement flap associated with M-plasty in the midline of the lower lip (Figure 3).
We made an incision in the skin following the lower edge of the surgical defect, close to the mental crease up to the left labial commissure. Then, we made an incision in the labial mucosa, respecting the height of the skin incision, to delimit the full-thickness myomucosal flap. We ensured that the inferior labial artery was contained within the flap, preserving its irrigation. No incision was made on the contralateral side (Figure 4).
Then, a full-thickness compensation triangle was removed in the middle portion of the mental crease, which was reconstructed with M-plasty to not invade the anatomical unit of the chin (Figure 5). We conducted the subsequent reconstruction in layers, respecting the mucosal, muscular, and cutaneous layers in that order. The compensation triangle was first reconstructed, and then the myomucosal flap was advanced and sutured. We used Vicryl® 5-0 in the reconstruction of the mucosa and Vicryl® 3-0 in the orbicularis oris muscle. The skin was sutured with 5-0 nylon thread (Figure 6).
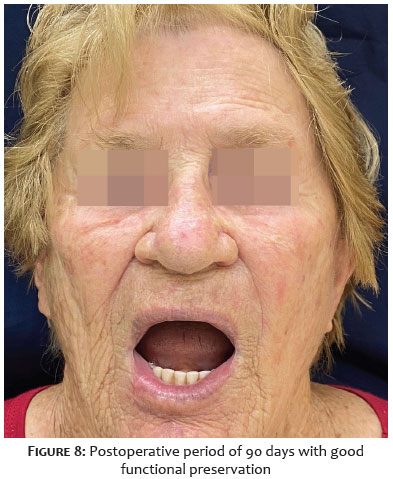
The patient evolved well, with little pain, edema, and bruising, in addition to excellent functional adaptation in the first days after surgery. In the three-month postoperative period, the patient presented perfect adaptation to the reconstruction without any aesthetic and functional damage (Figures 7 and 8).
Lower lip reconstruction aims mainly at the maximum preservation of functionality associated with minimal aesthetic impairment. Thus, some principles must be considered: correct reconstruction of the mucosal, muscular, and cutaneous planes; preservation of local vascular and nervous bundles; respect for anatomical units and subunits; maintenance of the proportion between the upper and lower lips; and perfect alignment of the transition zone between the vermilion and the skin.4
The literature describes and classifies (according to the proportion of site involvement) several techniques to reconstruct the lower lip with full-thickness defects. Surgical defects not exceeding 30% of involvement are treated by primary closure as wedge resection, Z-plasty, or M-plasty.2 Surgical defects larger than 30% require more complex reconstructions to avoid relevant aesthetic and functional complications, and local flaps are the best alternatives. In patients with total thickness tissue loss of around 45%, as in the present case, the surgical techniques classically described are bilateral myomucosal advancement, or Karapandzic flaps, and Gillies rotation flaps.3
The basic foundation of the myomucosal advancement flap is the existence of a greater amount of tissue in the lip vermilion than in the cutaneous portion of the lip. This flap provides good camouflage of the incision lines and preservation of neural and vascular structures. Also, it’s easy to perform and has low morbidity.5 Despite the literature describing the procedure for the closure of 45% of defects, in the present case, the isolated unilateral myomucosal flap couldn’t reconstruct the operative defect safely and without tension. Combining the myomucosal advancement flap and the M-plasty facilitated flap advancement, providing less tension on the surgical wound and, consequently, a lower risk of dehiscence and necrosis. Also, the associated M-plasty prevented the extension of the incision to another local anatomical unit.6
The Karapandzic and Gillies flaps are consecrated in large surgical defects in the lip reconstruction. However, these techniques require a greater learning curve by the surgeon and have relevant operative morbidity. They are based on the anatomical preservation of facial vascular-nervous pedicles, maintaining local irrigation and sensitivity. At the same time, they require extensive lines of incision and detachment, and their main complication is the risk of microstomia.2 In the case presented, we used two techniques that are easy to perform, have a shorter learning curve, and are mastered by most surgeons. They also present the technical advantage of the confinement of tissue movement in the anatomical unit of the lip.
Combining the myomucosal advancement flap with M-plasty proved to be a good alternative to reconstruct the full-thickness surgical defect of the lower lip with 45% involvement. Both techniques are easy to perform, present low morbidity, have a simple postoperative period, and, when associated, contribute to greater flap mobility and excellent aesthetic and functional results.
Liza Castro Rego
ORCID: 00-0001-7757-3278
Study design and planning; preparation and writing of the manuscript; collecting, analyzing, and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the literature; critical review of the manuscript.
Nathalia Calado Melges
ORCID: 09-0005-7158-9574
Study design and planning; preparation and writing of the manuscript; collecting, analyzing and interpreting data; critical review of the literature; critical review of the manuscript.
José Matheus Frizzo Lopes Moço
ORCID: 00-0001-8807-5717
Approval of the final version of the manuscript; preparation and writing of the manuscript; collecting, analyzing and interpreting data; critical review of the manuscript.
Thais Teixeira Libonati
ORCID: 09-0008-1647-8048
Preparation and writing of the manuscript; obtaining, analyzing and interpreting data; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
José Antonio Jabur da Cunha
ORCID: 00-0002-5780-0653
Approval of the final version of the manuscript; study design and planning; elaboration and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical review of the manuscript.
1. Pereira PMR, Rodrigues CAC, Lima LL, Romero SAR. Reconstrução do lábio inferior com técnica de Camille Bernard após excisão de carcinoma basocelular infiltrativo. Surg Cosmet Dermatol. 2013;5(1):81-3.
2. Contin LA, Carvalho MM, Machado Filho CDS, Hayashida ME, Ferraz TS, Gonçalves BF Jr. Reconstrução do lábio inferior com retalhos de Karapandzic e Gilles após excisão de carcinoma espinocelular. Surg Cosmet Dermatol. 2012;4(2):195-9.
3. Faulhaber J, Gérard C, Goerdt S, Koenen W. Functional and aesthetic reconstruction of full-thickness defects of the lower lip after tumor resection: analysis of 59 cases and discussion of a surgical approach. Dermatol Surg. 2010;36(6):859-67.
4. Faveret PLS. Lip reconstruction after tumor resection. Rev Bras Cir Plást. 2015;30(2):206-18.
5. Siqueira EJ, Alvarez GS, Laitano FL, Martins PDE, Oliveira MP. Estratégias em reconstrução do lábio inferior. Rev Bras Cir Plást. 2012;27(4):536-41.
6. Baker SR. Retalhos locais em reconstrução facial. 2nd ed. Rio de Janeiro: Di Livros; 2009.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}