


Daniela Alves Pereira Antelo1; Isabella Tartari2; Jaci Maria Santana3; Ursula Metelmann4; Isabela Bussade5; Jardis Volpe6
Financial support: L'Oréal Brasil provided funds for the authors' group meeting.
Conflict of interest: None.
Submitted on: 31/03/2023
Approved on: 05/05/2023
How to cite this article: Antelo DAP, Tartari I, Santana JM, Metelmann U, Bussade I, Volpe J. Impacts of exposome on the skin of menopausal women: from physiology to management. Surg Cosmet Dermatol. 2023;15:e20230240.
Hormonal changes added to extrinsic exposure factors, including socio-environmental and lifestyle factors, affect the quality of life of climacteric women. Symptoms during the climacteric are variable, and most women are not aware that menopause affects the skin. Among the perceived changes, there is an increase in dryness, roughness, sagging, and atrophied skin. This article reviews the relationship between exposure and menopause, focusing on helping dermatologists to guide patients on preventive care and treatments to improve skin and quality of life in menopause.
Keywords: Menopause; Perimenopause; Postmenopause; Climacteric; Exposome; Skin aging
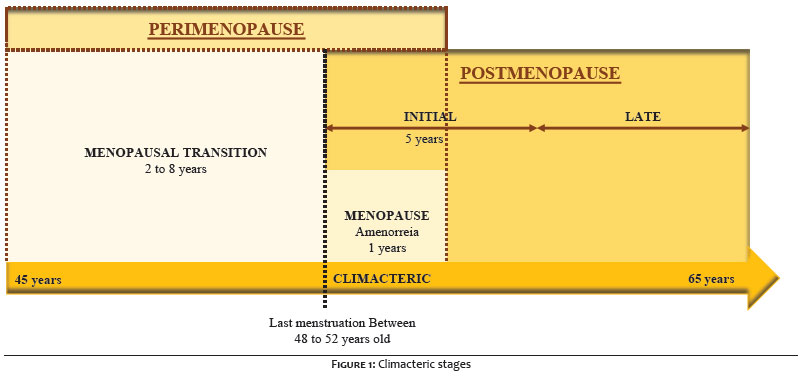
Menopause is recognized retrospectively, after 12 consecutive months of amenorrhea, and defined as the permanent interruption of menstruation, which inevitably occurs in all women, usually between 48 and 53 years of age.1,2 In Brazil, the average age of occurrence of natural menopause is 51.2 years3 and is usually preceded by a course of perimenopause, a period that extends from the menopausal transition to one year after menopause, which is usually more symptomatic due to hormonal oscillations (Figure 1).4,5
Age at menopausal transition, signs, and symptoms related to menopause are multifactorial and influenced by intrinsic and exposure factors, including socio-environmental and lifestyle factors.6–8
With the increase in Brazilian life expectancy, women spend more than a third of their lives in the postmenopausal phase.4 Thus, searches to maintain quality of life during the climacteric, moment when changes occur in the body and social, affective,3 sexual, family, and occupational life are essential.2,4
Therefore, this literature review aims to relate the impact of exposure factors on physiology to clinical dermatological manifestations during menopause, in addition to suggesting some practical guidelines for the management of these patients.
The physiological basis of clinical manifestations in menopause is complex and related, above all, to hormonal changes, in particular the reduction in the level of estrogenic hormones.7,9,10
The decrease in primordial follicles in the ovaries throughout life changes the hypothalamic-pituitary-ovarian axis, leading to a reduction in the production of inhibin B, estradiol, and progesterone.5,7,9
Lower production of inhibin B, whose normal function is to inhibit the secretion of follicle-stimulating hormone (FSH), causes an acceleration in follicular development, leading to shortening of menstrual cycles and irregular ovulation in the menopausal transition period.5,9
As menopause approaches, ovarian production of estradiol and anti-Müllerian hormone (AMH) – which reflects the ovarian follicular reserve – decreases. Withal, production of androstenedione and testosterone remains unchanged at the onset of menopause, contributing substantially to increasing circulating testosterone levels for about ten years.5,9
In postmenopause, FSH and luteinizing hormone (LH) tend to increase while the estradiol concentration decreases by up to 80%, with estrone becoming the predominant circulating estrogen.5 Decreased concentrations of sex hormone-binding globulin (SHBG - which binds specifically to testosterone and estradiol) exacerbates an imbalance between estrogens and androgens after menopause, increasing free androgen levels subsequently.9,10
Decreased progesterone increases the impact of androgen hormones on the sebaceous gland and hair follicle.4,9
In peripheral tissues, dehydroepiandrosterone (DHEA) and its sulfated metabolite (DHEA-S) can be converted intracellularly to more potent androgens or estrogens.9,11
About 75% of estrogen production in women occurs in peripheral tissues during pre-menopause and almost 100% in postmenopause.12
After menopause, skin and blood vessel cells, in addition to peripheral tissues, become sites of major estrogen synthesis.11,12
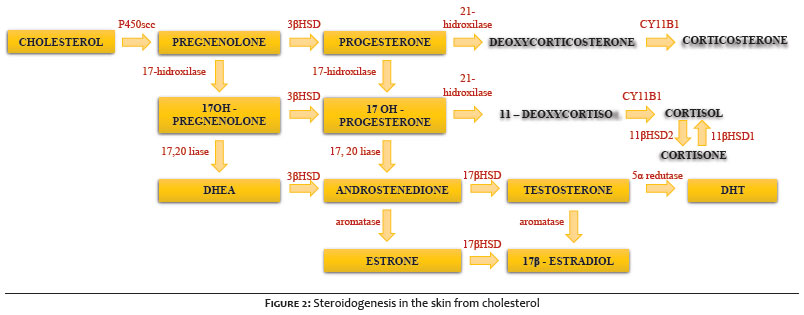
Although steroidogenesis in non-classical tissues is modest, cutaneous cells produce and regulate corticotropin-releasing hormone (CRH) peptides, in addition to other hormones such as IGF-1, thyroid-stimulating hormone (TSH), insulin-like growth factor 1 (IGF-1), vitamin D3, catecholamines, acetylcholine, serotonin, and melatonin.12–14
Figure 2 schematizes the cutaneous steroidogenic pathways from cholesterol.
Furthermore, the skin is the major non-reproductive target on which estrogen acts through binding to its alpha and beta receptors (ERα and ERβ), expressed by keratinocytes and fibroblasts,14,15 and the receptor G protein-coupled membrane estrogen (GPER1).7,10,16
The skin has a neuroendocrine system integrated with the cutaneous immune system through pro- and anti-inflammatory neuropeptides, cytokines, and hormones to preserve the structural integrity and barrier function.12 The decrease in estrogen levels during perimenopause has been associated with immunological changes, including increased secretion of pro-inflammatory cytokines (IL-1, IL-6, TNF-alpha), decreased production of anti-inflammatory cytokines (IL-10), and reduced ability to respond to pathogens.12,13
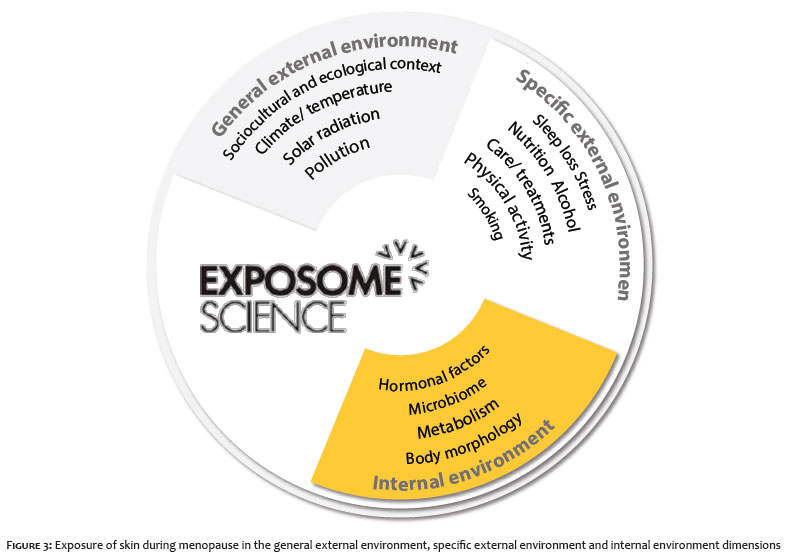
In addition to genetic factors, the primary exposomal factors involved in menopause can be systematized based on the three dimensions of exposome science: internal, general external, and specific external (Figure 3).17
Most women who have experienced the menopausal transition and postmenopause report several symptoms resulting from internal and constitutional factors, such as body composition, metabolism, and hormonal changes.13,18
In general, sex hormones decrease with advancing age and influence intrinsic skin aging, leading to cellular senescence, telomere shortening, decreased cellular proliferative capacity, chronic inflammation, mitochondrial DNA damage, and increased free radicals.19
There is a strong correlation between the estrogen deficiency that occurs with menopause and the loss of cutaneous collagen.8,20 In the first five years after the menopause milestone, there is a very accelerated loss of collagen (up to 30%), with great clinical repercussions, and the total collagen I and III decreases at an average rate of 2.1% per year in postmenopausal women over 15 years.6,9,21 Most studies suggest that the loss of collagen is more closely related to postmenopausal age than chronological age and therefore reflects hormonal effects.6,9,15,20
Accelerated degenerative changes in elastic fibers have been observed in women with premature menopause,6,20 with a 1.1% increase in facial skin distensibility and a 1.5% decrease in elasticity per year.21 In postmenopausal women, a gentle stretch of the skin on the back of the hand can take three to four times longer to reconstitute than in premenopausal women due to the arrangement alteration of fibers in the interface between epidermis and dermis caused by the reduced collagen expression and elastin degradation, in addition to the lack of glycosaminoglycans (GAGs), proteoglycans (PGs), and low dermis hydration.16,22 The loss of these components increases rigidity and decreases elasticity in the dermis.6,16 The skin elasticity appears to decrease at a rate of 1.5% per year in postmenopausal women.9
The decrease in GAGs with age alters the water content in the extracellular matrix and, in addition to increasing transepidermal water elimination, contributes to dryness, wrinkles, and skin atrophy.6,20
At the end of perimenopause, the level of estrogens decreases significantly, altering the ratio between estrogens and androgens and favoring androgenic activity, with a temporary increase in oiliness. In the postmenopausal period, on the contrary, the sebum level decreases sharply as a result of several biochemical changes, including a drop in the testosterone level.4,6,9 The postmenopausal decline in sebaceous gland activity may also contribute to skin dryness, one of the most common dermatological conditions in postmenopausal women.6 In tropical countries, such as Brazil, the climate favors the persistence of facial oiliness even in mature skin. Thus the high frequency of patients with a combination of oily skin,23 because the loss of skin hydration tends to occur first in the body area and is noticed later in the face.6
The influence of sex hormones on sebum production also affects the skin surface pH, which increases significantly with age, impairing the skin barrier function.4,24 The skin barrier function is damaged mainly by epidermis atrophy due to decreased activity of the basal layer and its close interaction with the dermis.1,24
In postmenopause, estradiol deficiency relates to lower defense capacity against oxidative stress, decreased skin water content, atrophy due to loss of collagen in the dermis, fine wrinkles with reduced skin elasticity, damage in the process of skin scarring, diminished vascularity, and hot flushes.25 Cutaneous changes aggravated by reduced microcirculation and atrophy of the postmenopausal dermal vascular network result in a reduced supply of nutrients and circulating hormones.9
The number of melanocytes also declines at a rate of 10–20% per decade of life in postmenopausal women, leading to a loss of uniformity in skin tone.5 Sometimes, the skin has mottled pigmentation.
From menopause, there is a reduction in the proliferative estrogen action in keratinocytes and fibroblasts in a scenario where there is a decrease in cell renewal with age, and the skin becomes more fragile and increasingly susceptible to trauma. While the characteristic premenopausal scars are more pigmented and raised, postmenopausal scars heal more slowly in response to decreased metabolic activity, with flatter, whitish scars.6,7
The impact of menopausal hormonal changes may be correlated with different races. Previous studies found that black skin has greater transepidermal water loss and intercellular cohesion within the stratum corneum, larger and more numerous fibroblasts with lower collagenase activity, melanocytes hyperactivity, and greater protection against solar radiation due to higher melanin content and melanosomes distribution in black skin compared to white.26 Therefore, significant racial differences in aging are observed mainly due to lower photodamage in black skin. The effect of hormones on the progression of skin aging in postmenopausal women was prospectively studied in different races, assessing wrinkles on the face and neck and skin tightness on the forehead and sides of the face.26 Black women had fewer wrinkles than white women in all four years of the study, with or without hormone replacement therapy, reinforcing the photoprotective role of melanin. On the other hand, black women showed a more significant decrease in total facial tightness after four years of follow-up than white women, although skin tightness had decreased in all groups. In that study, hormone therapy did not appear to affect wrinkles or skin tightness in most face areas.26
In the general external context, several psychosocial changes of an affective, sexual, family, or occupational nature, can occur during the menopausal transition.2,27 Changes in body composition and fat distribution, even in cases without changes in body weight, can affect self-image and potentiate mood disorders that vary according to the culture of each society about female aging.2 Factors such as body image, interpersonal relationships, sociocultural status, and the role of middle-aged women can influence women's behavior about menopause and impact their perception of the intensity of the symptoms. Studies have shown that women who are dissatisfied with their appearance have more menopausal symptoms.19
In countries with a high incidence of UV radiation, such as Brazil, it is necessary to balance the benefits and harms linked to sun exposure.8,25,28 In postmenopausal women, a large-scale epidemiological study observed that greater exposure to UV radiation was associated with lower levels of estradiol and estrone and elevated levels of FSH and LH. One of the mechanisms to explain the negative association between estrogens and UV radiation is based on the metabolism of vitamin D and its storage in adipose tissue, the primary site of estrogen production in postmenopausal women.29
In addition to UV radiation, new evidence suggests that environmental pollution, particularly by persistent organic pollutants, can interfere with the endocrine system and affect the synthesis of steroid and thyroid hormones, in addition to inhibiting the activity and expression of cytochrome P450 and, indirectly, cause vitamin D deficiency.14
A stressful routine and sleep deprivation form a vicious cycle, since stress, in addition to contributing to a pro-inflammatory state, causes an increase in cortisol levels, which delays the onset of sleep.25
The loss of sleep architecture, sleep fragmentation, and early awakening are phenomena well characterized in the menopausal transition, linked to lower melatoninergic production and, in part, to the reduction of serum estrogen. The prevalence of sleep disorders in perimenopausal women ranges from 39% to 47%.30 These conditions disturb the circadian rhythm and lead to cell dysfunction, causing systemic effects and inducing skin changes.8,30 Sleep deprivation for a long time can alter cutaneous healing processes and the immune response, promoting the degradation of the dermal matrix.25
Cortisol and pro-inflammatory cytokines impair collagen fiber production and integrity through glucocorticoid-mediated processes, increase extracellular matrix metalloproteinase (MMP) activity, promote water loss, and damage the DNA.19
The activation of endogenous glucocorticoids, mediated by an increased expression of 11β-hydroxysteroid dehydrogenase-1 (11β-HSD1), increases the level of cortisol in the skin, inhibiting the keratinocytes differentiation, and decreases the cytokines expression necessary for maintaining skin barrier function.18
In response to the psychobiological burden of menopause, cortisol plays an important role, and its production increases during the final stage of the menopausal transition, leading to hypercortisolism associated with poorer endothelial quality.18,31
New biomarkers were identified in the stratum corneum of postmenopausal skin, with a significant increase in calmodulin-like skin proteins, desmoglein 1, junction plakoglobin, and heat shock protein, which can affect the process of epidermal desquamation, with an accumulation of cells in the skin stratum corneum. On the other hand, levels of transglutaminase-3, apolipoprotein D, and acid ceramidase were significantly reduced in the postmenopausal stratum corneum, probably reflecting reduced sweat secretion and drier skin.15,25
Another significant factor that leads to premature skin aging is smoking. For some authors, smoking contributes more to the formation of facial wrinkles than sun exposure.14 Major changes occur mainly in the dermis, resulting in collagen degeneration, deposition of abnormal elastic material, increase in dysfunctional GAGs and PGs, and vessel dilation with thickening of the walls. In the epidermis, smoking increases keratinocyte dysplasia and skin roughness in a relationship dependent on the amount of exposure to tobacco smoke.14 A study with 730 postmenopausal women divided into groups according to their smoking status (current smokers, former smokers, never smokers) showed that hormone replacement therapy (HRT) did not improve facial wrinkle scores in smokers but improved wrinkles in non-smokers. It suggests that facial skin damage caused by long-term tobacco use may not be reversible with estrogen therapy.14
During perimenopause, emotional lability and anxiety increase a woman's risk of developing binge eating disorders, which may be accompanied by a change in taste perception and predilection for sweets/carbohydrates, favoring hyperglycemia and obesity associated with metabolic dysfunction.2,5,9 Excessive food consumption or ingestion of sugars and processed carbohydrates tend to be the main contributors to the formation of advanced glycation end products (AGEs), as they impact glycation, which is the non-binding enzymatic blending of sugars with proteins. AGEs affect the bonds between collagen fibers, reducing the elasticity of the skin and the inner walls of blood vessels, predisposing to age-related chronic diseases such as hypertension and cardiovascular disease.25
Studies with climacteric women aged >40 years have shown, among other factors, that practicing physical exercises in open or closed environments less than two to three times a week and frequent sleep deprivation were potential risk factors for facial wrinkles.32
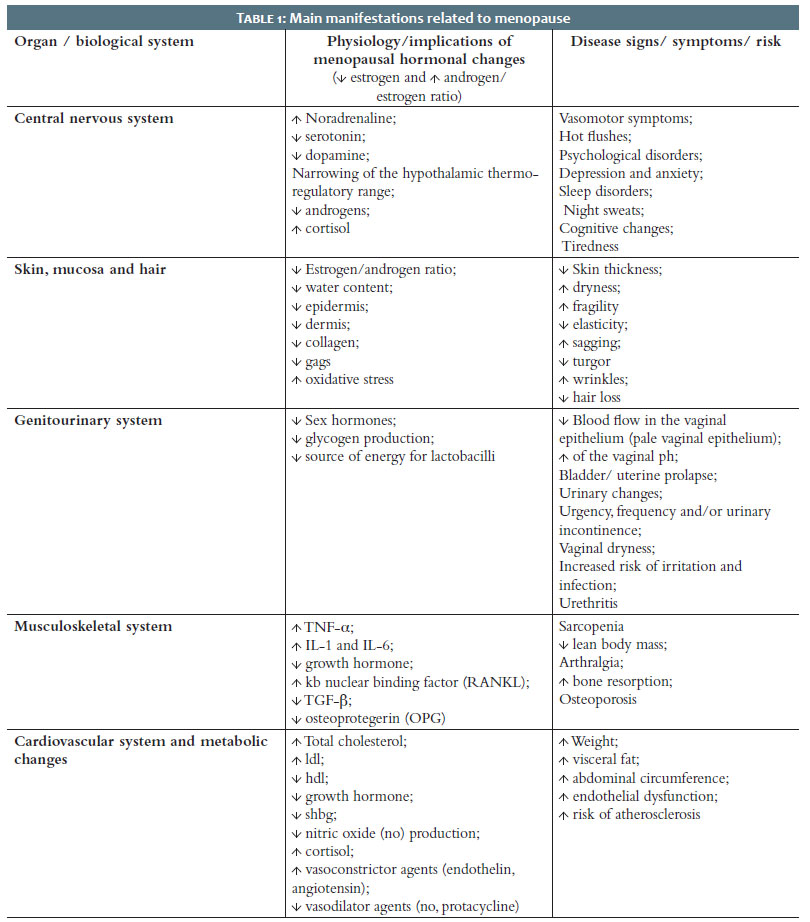
Symptoms during the climacteric vary in different women and may affect one or more systems (Table 1).2,9 The most common symptoms (75% of women) that often lead women to medical consultations are vasomotor symptoms. (VMS).9,33
Skin symptoms often receive less attention than other menopause symptoms because most women are not aware that menopause affects the skin.34
Clinical experience reveals that women are unaware of most menopausal symptoms, especially the earlier ones. Also, patients ignore the impact of the menopausal transition.
A survey of 1,287 French women (476 women in menopause; 811 women in the reproductive stage) highlighted the need for information about menopause since 67% of women in the reproductive period and 50% of women in menopause declared they were not sufficiently informed about menopause.34
Thus, it is essential to comprehend how to guide the patient to a better understanding of this physiological transition and how to manage the signs and symptoms during menopause so that women can have a better quality of life.2
Individual and collective guidelines for women approaching menopause become increasingly significant given the longevity perspective. Thus, a practice that encourages a healthy lifestyle is recommended.2 Currently, digital tools and social networks enable scientific dissemination and educational activities for menopausal women, a public that is very interested in guidelines. Videos, podcasts, and digital pamphlets are available to this audience on the websites of national medical associations and specific international societies, such as the International Menopause Society (IMS; www.imsociety.org), aiming to promote education and research on middle-aged women's health.
Nutrition and oral supplementation
From the health promotion perspective, menopause demands a change in diet regarding the macronutrients that impact the skin.35,36 It is essential to increase the supply of proteins, seek sources of specific amino acids, such as cysteine, lysine, and tryptophan, and avoid excess sweets and refined carbohydrates that raise glucose and contribute to developing type 2 diabetes.5 Oral supplements and nutraceuticals can be included to complement the dietary nutrients of the menopausal woman.5
In postmenopause, supplementation with amino acids is also necessary to maintain muscle mass. A leucine metabolite, β-hydroxy β-methylbutyrate (HMB), has been used with good clinical results, helping to gain lean mass. Oral supplementation with arginine, glutamine, and HMB for four weeks in sedentary postmenopausal women reduced visceral fat and improved skin texture, probably by increasing collagen.37 The ingestion of bioactive peptides can also stimulate collagen in general specific dipeptides and tripeptides obtained from collagens from different sources.38,39
Foods rich in phytoestrogens (isoflavones and lignans) help to minimize the negative impact of hormonal changes in menopause. Despite the structural and functional homology with estradiol, which leads to the assumption of interaction with estrogen receptors, phytoestrogens have a subtle effect.40
Omega-6 and omega-3 are essential fatty acids whose main food source is fish oils.38 Their low consumption can affect the composition of the epidermis, cause increased transepidermal water loss and a deficiency in the skin barrier function, in addition to increasing proliferative keratins (K6 and K16) and inflammation-related keratin (K17).36,38,39
Coenzyme Q10 (CoQ) supplementation has been shown to partially prevent cardiovascular and brain damage due to its bioenergetic and antioxidant effects, with evidence indicating its action in restoring mitochondrial activity and reducing cognitive decline in postmenopausal women. CoQ found in the dermis, epidermis, and stratum corneum lipids decreases with age and UV exposure, and its replacement is crucial in improving skin characteristics in intrinsic aging and the climacteric.41 Another antioxidant related to vascular benefits for women in menopause is Pinus pinaster extract, used mainly in pigmentary changes in the skin.39
Meat, liver, mushrooms, vegetables, nuts, green vegetables, whole grains, tea, and coffee are sources of nicotinamide that prevent the depletion of cellular NAD+, with an increase in cellular energy that contributes to the DNA repair process.25
The identification and treatment of vitamin D deficiency in postmenopausal women can improve their general health, being particularly interesting due to the high prevalence of musculoskeletal disorders in this phase, in addition to changes in metabolism and body composition that affect the cutaneous synthesis of vitamin D, its physiological function, and prevention of osteoporosis.27 A cross-sectional study with perimenopausal and postmenopausal Thai women compared the level of vitamin D between an outdoor working group and an indoor working group. Vitamin D levels in perimenopausal and postmenopausal women were low, with a high prevalence of vitamin D insufficiency in both groups, signaling the importance of oral supplementation even in menopausal women who work outdoors.42
One should also avoid the consumption of alcoholic beverages, excessive caffeine, and spicy foods, such as black pepper, which contains piperine, and cinnamon, which contains cinnamic aldehyde, as they cause vasodilation and can trigger the worsening of hot flushes and the appearance of rosacea.25
Regular engagement in physical activity recruits microcirculation, positively impacting skin health, cardiorespiratory fitness, and decreasing hot flushes.2,32 In addition to reducing the severity of vasomotor symptoms, physical activity increases irisin production, improves the quality of life in the climacteric, and may play an essential role in reducing depression and improving body image perception.35
Practicing 150 minutes of moderate-intensity aerobic activity per week should be encouraged, in addition to muscle strengthening.2,5 Pelvic gymnastics and Kegel exercises help strengthen the pelvic floor and vaginal muscles and may prevent incontinence and urinary urgency.5
Menopausal women should practice leisure activities, relaxation, motor coordination, balance, and socialization whenever possible. Breathing exercises or oriental activities such as meditation and yoga provide physical and psycho-emotional well being.5
Self-care improves self-esteem and insecurity in the face of changes inherent to menopause. Among the guidelines, water intake; six to eight hours of adequate sleep; skin and hair cleansing and moisturizing care; avoiding smoking and hot, poorly ventilated environments are recommended.5
The benefits of hormone therapy within 36 months of the last menstrual period in women aged 50 to 60 years include managing menopausal vasomotor symptoms, reducing osteoporotic fracture risk, and improving quality of life (which may have a cardioprotective effect).1,25 Moreover, the increased risk of developing thromboembolism outweighs the benefits in advanced postmenopausal women.25 The risks vary according to the type, dose, duration, route of administration, time of onset, and use or not of progestogen. Ideally, the treatment should be individualized and accompanied by a gynecologist or endocrinologist.1 In women aged <60 years or within ten years of the onset of menopause with no formal contraindications, the risk-benefit ratio is more favorable. Several studies suggest the use of systemic and topical estrogen. Most demonstrate positive effects, increasing the skin's collagen content, thickness, elasticity, and hydration and decreasing menopausal vaginal dryness. Despite encouraging results, the anti-aging indication alone does not justify systemic estrogen therapy due to potentially serious adverse events and still controversial skin outcomes.4
Topical estrogen preparations provide a more specific therapeutic option for anti-aging goals and don't increase the systemic estrogen level effects at experimental doses of 0.01% estradiol and 0.3% estriol.4,15
2% progesterone cream improves skin elasticity and reduces the amount and depth of wrinkles in perimenopausal and postmenopausal women. However, progesterone is highly absorbed by tissues. Thus the topical application effects are likely to become systemic.43
Local application of DHEA significantly increases the expression of androgen receptors, procollagen I and III, and heat shock protein 4, necessary for collagen synthesis in the dermis, while modulating keratinocyte differentiation.25,43
Topical dermatological treatments
When choosing an effective dermocosmetic routine, it is necessary to combine the needs of perimenopausal and postmenopausal skin with the right active ingredients.
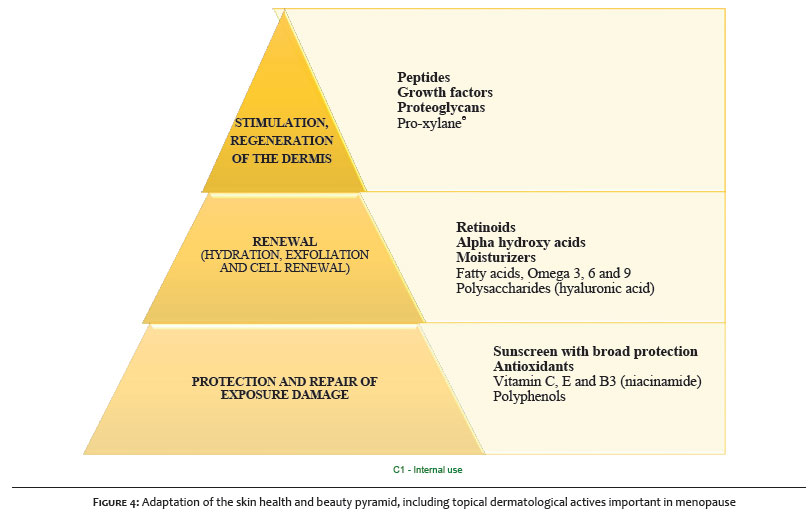
For a hierarchically organized approach, the most relevant actives in menopause are presented below (Figure 4), through an adaptation to the "Skin health and beauty pyramid" in which the base of the pyramid represents the indispensable for daily care; the middle represents what is needed to help with the transformation; and the top represents the additional, but crucial to cellular stimulation.44
The base of the pyramid encompasses actives for protecting and repairing skin against damage caused by exposure factors, including sun protection and antioxidants that play an essential role in the face of aging aggravated by sex hormones, especially during perimenopause and the beginning of postmenopause (first five years).8,25
Women should use a broad-spectrum (UVB, UVA1/UVA2) sunscreen daily to reduce photodamage to the skin.8
Regarding antioxidants, the topical use of vitamins C, E, and B3 (niacinamide) and polyphenols is recommended.
Vitamin C (pure L-ascorbic acid) in concentrations ranging from 5% to 15% has a topical anti-aging effect by inducing the production of collagen I, collagen III, and enzymes important in collagen production and metalloproteinase-1 inhibition.43
Vitamin E (tocopherol) protects the skin from the adverse events of oxidative stress induced by UV, visible light, infrared, and pollution in in vitro tests.43
Topical vitamin B3 (niacinamide) regulates cell metabolism and skin regeneration, reducing the inflammatory response with anti-aging and depigmenting effects by inhibiting the transfer of melanosomes from melanocytes to keratinocytes.43,44
The topical application of polyphenols is essential in menopause due to their antioxidant, anti-inflammatory, and immunomodulatory effects.40,43 The topical effects of isoflavones on the skin of postmenopausal women show improved dryness, increased thickness, decreased facial wrinkles, greater fibroblast viability, augmented hyaluronic acid concentration, and collagen types I and III production.40,43
The benefits of resveratrol, a non-flavonoid polyphenol, include anti-inflammatory and antioxidant properties that protect against UV radiation and oxidative stress, reduce the expression of transcription factors AP-1 and NF-kB, and the proliferation of fibroblasts to increase the collagen types I, II and III, inhibit melanogenesis, and activate sirtuin 1.18
The middle of the pyramid considers transforming actives, with cell renewal and moisturizing action.
Retinoids are renewing actives recognized for their ability to induce collagen synthesis and reduce MMP-1 expression. Tretinoin is the reference retinoid to reduce the signs of UV-induced skin aging, such as wrinkles, loss of skin elasticity, and pigmentation. It has been used in climacteric women, accompanied by adequate care for recovery and protection of the skin barrier.19,43 Retinoids, especially tretinoin, increase the potential for steroid hormone production in many classic and non-classical steroidogenic tissues, reduced by hormonal imbalance in the climacteric. The local regulation of steroidogenic activity in keratinocytes is vital for the physiology and homeostasis of the skin.14 Retinol has been widely used as an anti-aging active, acting on collagen metabolism, because, compared to tretinoin, it causes less skin irritation. Treatment with a 0.4% retinol formulation increased total skin GAGs as determined by immunostaining.22,43
Topical treatment with AHA assists skin cell renewal and stimulates an increase in GAGs and hyaluronic acid, correlated with better skin quality and hydration. The main active of this group is glycolic acid, which, in addition to its renewing action, evens skin tone and texture.22
During and after the menopausal transition, the skin needs to recover its water content substantially.21 The most important topical actives are vegetable oils extracted from sunflower, apricot, argan, coconut, shea, and rice bran seeds, which stand out for their high omega-3, omega-6, and omega-9 concentrations. Vegetable oils activate epidermal lipogenesis and help repair the body or facial skin barrier.38
Fatty acids play fundamental roles in inflammatory responses, either in the form of cell membrane phospholipids or as soluble lipoic mediators, with evidence of skin healing modulation. Omega-9 fatty acids heal wounds faster than others. In addition to accelerating healing, omega-3 and omega-6 polyunsaturated fatty acids may improve skin barrier function, inhibit UV-induced inflammation and hyperpigmentation, and alleviate skin dryness. Linoleic acid, a fatty acid from the omega-6 family, is the most important in the epidermis and stimulates the synthesis of ceramides. Omega-3 fatty acids can modify the immune response of the epidermis via T cells, acting on toll-like receptors and stimulating caspase cascades that alleviate inflammatory dermatoses.38
Topical administration provides a direct and efficient way to deliver polyunsaturated and monounsaturated fatty acids to the skin with greater bioavailability than the oral route.38
Polysaccharides are essential actives for the dermis of peri and postmenopausal women, who need to increase the GAGs content to recover turgor and reduce skin flaccidity. The most widely known class of GAGs is hyaluronic acid (HA).44 Daily use of formulas containing HA results in reduced wrinkle depth, slackness, and skin dehydration with increased barrier function, being a safe active. High molecular weight HA does not penetrate the skin. However, preparations containing HA fragments of varying sizes may improve skin penetration.22
The seeds of the Indian plant Cassia angustifolia provide a polysaccharide capable of producing intense hydration in the epidermis, leaving the skin luminous, in addition to modulating the expression of 11β-HSD1 in keratinocytes in vitro and reducing the synthesis of cortisol in the skin. In fibroblasts, cassia extract prevents the action of cortisol in reducing collagen and restores the synthesis of hyaluronic acid, contributing to skin hydration.45,46
The top of the pyramid encompasses actives that stimulate and benefit the dermis in search of firmness and density, the primary skin issues in menopause.44
Pro-xylane® is a C-xyloside that initiates and stimulates the production of GAGs in the dermis, being able to redensify this compartment, increasing the water content in the skin extracellular matrix. At the dermal-epidermal junction, Pro-xylane® stimulates the synthesis of basement membrane anchoring microfilaments (collagen IV, collagen VII, and laminin 5) and components of the papillary dermis (procollagen I, fibrillin 1), strengthening adhesion and cohesion between layers. Consequently, it increases skin density and accelerates the movement of growth factors and nutrients, leaving menopausal skin more hydrated.44,47 A clinical study comparing a dermocosmetic containing 3% Pro-xylane® versus a moisturizing cream in 238 women in postmenopause, during 60 days of daily application, showed a significant improvement in skin firmness, density, brightness, and homogeneity.48
Polypeptides (chains of amino acids) can stimulate collagen synthesis and activate dermal metabolism through topical application.43 The three main families are signal inhibitors, transporters, or neurotransmitter peptides.44
Menopausal patients demand aesthetic procedures, probably impacted by structural changes in the skin. Botulinum toxin, fillers, peelings, laser, microfocused ultrasound, and radiofrequency can help these patients face this period, improving skin quality.43 Skin and mucosal procedures in the genitourinary region in search of functional health and beauty are gaining space to improve muscle tone and support. Filling of the labia majora, peeling, vaginal laser, and radiofrequency are conducted, in addition to the administration of topical products for adequate hydration of the region.49
Menopause is a biological phenomenon in which estrogen deficiency occurs, affecting physiological and biological functions in many organs, including the skin, which denotes a qualitative decline in their physical characteristics.6,7,9 As a result, women in menopause usually present issues with the aging process, a drop in self-esteem, and demand for dermatological treatments that improve self-image and quality of life.16,38,40,43,50
The dermatologist must play an active role in the prevention and care of facial and extra-facial skin, conducting interventions to stimulate collagen formation and improve skin support. These processes must start already in perimenopause. Knowing the patient's lifestyle from age 40 can contribute to general guidelines and facilitate managing exposure factors and choosing products according to each reality. In an integral view, it is necessary that the dermatologist welcomes the patient and directs her, whenever necessary, for parallel follow-up with other specialists, such as an endocrinologist and/or gynecologist, also verifying the relevance of hormone therapy.
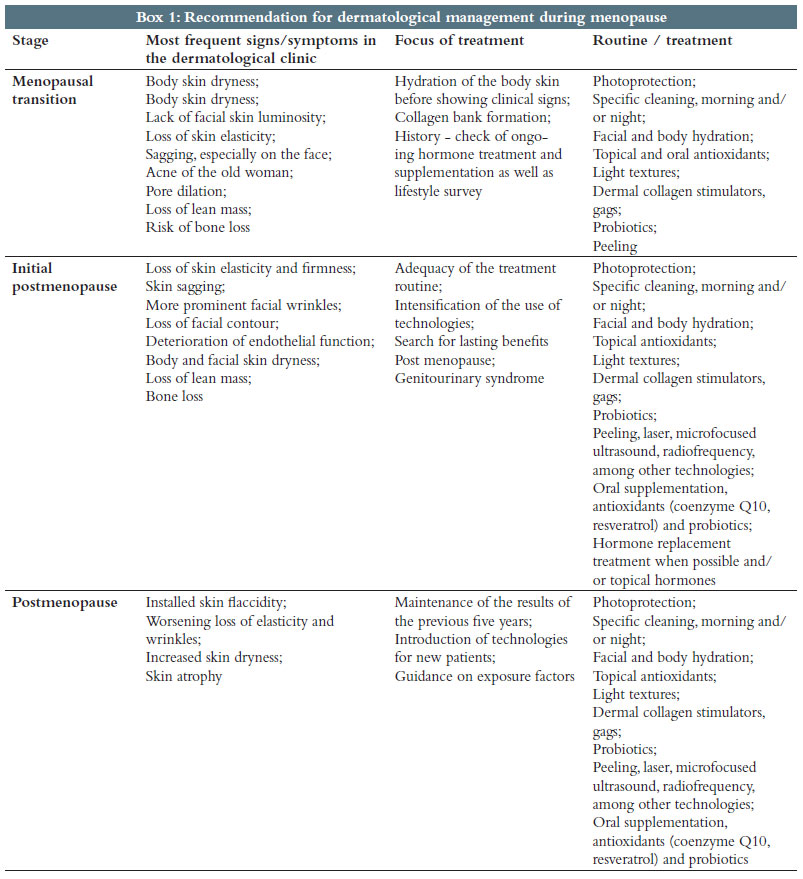
Based on their clinical experiences, the authors suggest a dermatologist's new look towards menopause, considering three very characteristic phases: perimenopause, initial postmenopause, and five years after menopause (Box 1), seeking to intervene and help the patient the best way in each of these phases.
Daniela Alves Pereira Antelo
ORCID: 0000-0001-8203-1772
Approval of the final version of the manuscript; active participation in research orientation; critical literature review; critical revision of the manuscript.
Isabella Tartari
ORCID: 0000-0001-8622-3595
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Jaci Maria Santana
ORCID: 0000-0003-2582-3751
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Ursula Metelmann
ORCID: 0000-0002-2446-6417
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Isabela Bussade
ORCID:0000-0002-7846-6789
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Jardis Volpe
ORCID: 0000-0002-2237-2636
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
1. The NAMS 2017 Hormone Therapy Position Statement Advisory Panel. The 2017 hormone therapy position statement of The North American Menopause Society. Menopause. 2017;24(7):728-53.
2. Ministério da Saúde, Instituto Sírio-Libanês de Ensino e Pesquisa. Protocolos da Atenção Básica: saúde das mulheres. 1st Ed. MS/CGDI; 2016.
3. Pedro AO, Neto AMP, Paiva LHSC, Osis MJ, Hardy E. Idade de ocorrência da menopausa natural em mulheres brasileiras. Cad Saúde Pública. 2003;19(1):17-25.
4. Duarte GV, Trigo AC, Oliveira Mde MFP. Skin disorders during menopause. Cutis. 2016;97(2):E16-23.
5. Secretaria de Atençãoà Saúde Departamento de Ações Programáticas Estratégicas. Normas Manuais Técnicos Série Direitos Sexuais Direitos Reprodutivos - Caderno SA; 2008.
6. Calleja-Agius J, Brincat M. The effect of menopause on the skin and other connective tissues. Gynecol Endocrinol. 2012;28(4):273-7.
7. Wilkinson HN, Hardman MJ. A role for estrogen in skin ageing and dermal biomechanics. Mech Ageing Dev. 2021;197:111513.
8. Krutmann J, Bouloc A, Sore G, Bernard BA, Passeron T. The skin aging exposome. J Dermatol Sci. 2017;85(3):152-61.
9. Monteleone P, Mascagni G, Giannini A, Genazzani AR, Simoncini T. Symptoms of menopause - global prevalence, physiology and implications. Nat Rev Endocrinol. 2018;14(4):199-215.
10. O'Neill S, Eden J. The pathophysiology of menopausal symptoms. Obstet Gynaecol Reprod Med. 2017;27(10):303-10.
11. Labrie F, Martel C, Bélanger A, Pelletier G. Androgens in women are essentially made from DHEA in each peripheral tissue according to intracrinology. J Steroid Biochem Mol Biol. 2017;168:9-18.
12. Slominski A, Zbytek B, Nikolakis G, Manna PR, Skobowiat C, Zmijewski M, et al. Steroidogenesis in the skin: implications for local immune functions. J Steroid Biochem Mol Biol. 2013;137:107-23.
13. Pondeljak N, Lugović-Mihić L. Stress-induced interaction of skin immune cells, hormones, and neurotransmitters. Clin Ther. 2020;42(5):757-70.
14. Bocheva G, Slominski RM, Slominski AT. Neuroendocrine aspects of skin aging. Int J Mol Sci. 2019;20(11):2798.
15. Archer DF. Postmenopausal skin and estrogen. Gynecol Endocrinol. 2012;28 Suppl 2:2-6.
16. Lephart ED, Naftolin F. Menopause and the skin: old favorites and new innovations in cosmeceuticals for estrogen-deficient skin. Dermatol Ther. 2021;11(1):53-69.
17. Wild CP. The exposome: from concept to utility. Int J Epidemiol. 2012;41(1):24-32.
18. Choe SJ, Kim D, Kim EJ, Ahn JS, Choi EJ, Son ED, et al. Psychological stress deteriorates skin barrier function by activating 11β-Hydroxysteroid dehydrogenase 1 and the HPA Axis. Sci Rep. 2018;8(1):6334.
19. Blume-Peytavi U, Atkin S, Gieler U, Grimalt R. Skin academy: hair, skin, hormones and menopause - current status/knowledge on the management of hair disorders in menopausal women. Eur J Dermatol. 2012;22(3):310-8.
20. Hall G, Phillips TJ. Estrogen and skin: the effects of estrogen, menopause, and hormone replacement therapy on the skin. J Am Acad Dermatol. 2005;53(4):555-68.
21. Brincat M, Muscat Baron Y, Galea R. Estrogens and the skin. Climacteric. 2005;8(2):110-23.
22. Wang ST, Neo BH, Betts RJ. Glycosaminoglycans: sweet as sugar targets for topical skin anti-aging. Clin Cosmet Investig Dermatol. 2021;14:1227-46.
23. Melo MO, Campos PM. Characterization of oily mature skin by biophysical and skin imaging techniques. Skin Res Technol. 2018;24(3):386-95.
24. Tončić RJ, Kezić S, Hadžavdić SL, Marinović B. Skin barrier and dry skin in the mature patient. Clin Dermatol. 2018;36(2):109-15.
25. Passeron T, Krutmann J, Andersen ML, Katta R, Zouboulis CC. Clinical and biological impact of the exposome on the skin. J Eur Acad Dermatol Venereol. 2020;34(Suppl 4):4-25.
26. Owen CM, Pal L, Mumford SL, Freeman R, Isaac B, McDonald L, et al. Effects of hormones on skin wrinkles and rigidity vary by race/ethnicity: four-year follow-up from the ancillary skin study of the kronos early estrogen prevention study. Fertil Steril. 2016;106(5):1170-5.
27. Pérez-López FR, Chedraui P, Pilz S. Vitamin D supplementation after the menopause. Ther Adv Endocrinol Metab. 2020;11:2042018820931291.
28. Passeron T, Bouillon R, Callender V, Cestari T, Diepgen TL, Green AC, et al. Sunscreen photoprotection and vitamin D status. Br J Dermatol. 2019;181(5):916-31.
29. Triebner K, Bifulco E, Barrera-Gómez J, Basagaña X, Benediktsdóttir B, Forsberg B, et al. Ultraviolet radiation as a predictor of sex hormone levels in postmenopausal women: a european multi-center study (ECRHS). Maturitas. 2021;145:49-55.
30. Lee J, Han Y, Cho HH, Kim MR. Sleep disorders and menopause. J Menopausal Med. 2019;25(2):83-7.
31. Kim BJ, Lee NR, Lee CH, Lee YB, Choe SJ, Lee S, et al. Increased expression of 11β-Hydroxysteroid dehydrogenase type 1 contributes to epidermal permeability barrier dysfunction in aged skin. Int J Mol Sci. 2021;22(11):5750.
32. Park S, Kang S, Lee WJ. Menopause, ultraviolet exposure, and low water intake potentially interact with the genetic variants related to collagen metabolism involved in skin wrinkle risk in middle-aged women. Int J Environ Res Public Health. 2021;18(4):2044.
33. Woods NF, Mitchell ES. Symptoms during the perimenopause: prevalence, severity, trajectory, and significance in women's lives. Am J Med. 2005;118(Suppl 12B):14-24.
34. LePillouer-Prost A, Kerob D, Nielsen M, Taieb C, Maitrot Mantelet L. Skin and menopause: women's point of view. J Eur Acad Dermatol Venereol. 2020;34(6):e267-9.
35. Namazi M, Sadeghi R, Behboodi Moghadam Z. Social determinants of health in menopause: an integrative review. Int J Womens Health. 2019;11:637-47.
36. Rietjens IMCM, Louisse J, Beekmann K. The potential health effects of dietary phytoestrogens. Br J Pharmacol. 2017;174(11):1263-80.
37. Rondanelli M, Nichetti M, Peroni G, Naso M, Faliva MA, Iannello G, et al Effect of a food for special medical purposes for muscle recovery, consisting of arginine, glutamine and Beta-Hydroxy-Beta-methylbutyrate on body composition and skin health in overweight and obese class I sedentary postmenopausal women. Nutrients. 2021;13(3):975.
38. Huang TH, Wang PW, Yang SC, Chou WL, Fang JY. Cosmetic and therapeutic applications of fish oil's fatty acids on the skin. Mar Drugs. 2018;16(8):256.
39. Pérez-Sánchez A, Barrajón-Catalán E, Herranz-López M, Micol V. Nutraceuticals for skin care: A comprehensive review of human clinical studies. Nutrients. 2018;10(4):403.
40. Rzepecki AK, Murase JE, Juran R, Fabi SG, McLellan BN. Estrogen-deficient skin: the role of topical therapy. Int J Womens Dermatol. 2019;5(2):85-90.
41. Cirilli I, Damiani E, Dludla PV, Hargreaves I, Marcheggiani F, Millichap LE, et al. Role of coenzyme Q10 in health and disease: an update on the last 10 years (2010-2020). Antioxidants. 2021;10(8):1325.
42. Wongkhankaew N, Pongsatha S. A cross sectional study of serum vitamin D levels in perimenopausal and postmenopausal women working outdoors or indoors. J Med Assoc Thai. 2021;104(11):1807-13.
43. Zouboulis CC, Ganceviciene R, Liakou AI, Theodoridis A, Elewa R, Makrantonaki E. Aesthetic aspects of skin aging, prevention, and local treatment. Clin Dermatol. 2019;37(4):365-72.
44. Draelos ZD. Revisiting the skin health and beauty pyramid: a clinically based guide to selecting topical skincare products. J Drugs Dermatol. 2021;20(6):695-9.
45. Sharma P, Sharma S, Ramakrishna G, Srivastava H, Gaikwad K. A comprehensive review on leguminous galactomannans: structural analysis, functional properties, biosynthesis process and industrial applications. Crit Rev Food Sci Nutr. 2022;62(2):443-65.
46. Zouboulis CC, Blume-Peytavi U, Kosmadaki M, Roó E, Vexiau-Robert D, Kerob D, et al. Skin, hair and beyond: the impact of menopause. Climacteric. 2022;25(5):434-42.
47. Vassal-Stermann E, Duranton A, Black AF, Azadiguian G, Demaude J, Lortat-Jacob H, et al. A new C-Xyloside induces modifications of GAG expression, structure and functional properties. PLoS One. 2012;7(10):e47933.
48. Bouloc A, Roo E, Moga A, Chadoutaud B, Zouboulis CC. A compensating skin care complex containing pro-xylane in menopausal women: results from a multicentre, evaluator-blinded, randomized study. Acta Derm Venereol. 2017;97(4):541-2.
49. Wańczyk-Baszak J, Woźniak S, Milejski B, Paszkowski T. Genitourinary syndrome of menopause treatment using lasers and temperature-controlled radiofrequency. Prz Menopauzalny. 2018;17(4):180-4.
50. Shifren JL, Gass ML; NAMS Recommendations for Clinical Care of Midlife Women Working Group. The North American Menopause Society recommendations for clinical care of midlife women. Menopause. 2014;21(10):1038-62.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}